

Discharge planning in chronic conditions: an evidence-based analysis
- PMID: 24167538
- PMCID: PMC3804053
Discharge planning in chronic conditions: an evidence-based analysis
Abstract
Background: Chronically ill people experience frequent changes in health status accompanied by multiple transitions between care settings and care providers. Discharge planning provides support services, follow-up activities, and other interventions that span pre-hospital discharge to post-hospital settings.
Objective: To determine if discharge planning is effective at reducing health resource utilization and improving patient outcomes compared with standard care alone.
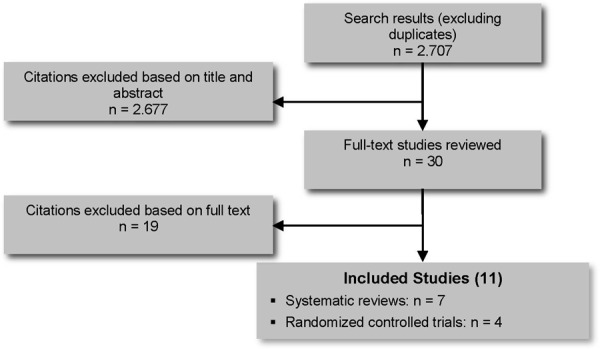
Data sources: A standard systematic literature search was conducted for studies published from January 1, 2004, until December 13, 2011.
Review methods: Reports, randomized controlled trials, systematic reviews, and meta-analyses with 1 month or more of follow-up and limited to specified chronic conditions were examined. Outcomes included mortality/survival, readmissions and emergency department (ED) visits, hospital length of stay (LOS), health-related quality of life (HRQOL), and patient satisfaction.
Results: One meta-analysis compared individualized discharge planning to usual care and found a significant reduction in readmissions favouring individualized discharge planning. A second meta-analysis compared comprehensive discharge planning with postdischarge support to usual care. There was a significant reduction in readmissions favouring discharge planning with postdischarge support. However, there was significant statistical heterogeneity. For both meta-analyses there was a nonsignificant reduction in mortality between the study arms.
Limitations: There was difficulty in distinguishing the relative contribution of each element within the terms "discharge planning" and "postdischarge support." For most studies, "usual care" was not explicitly described.
Conclusions: Compared with usual care, there was moderate quality evidence that individualized discharge planning is more effective at reducing readmissions or hospital LOS but not mortality, and very low quality evidence that it is more effective at improving HRQOL or patient satisfaction. Compared with usual care, there was low quality evidence that the discharge planning plus postdischarge support is more effective at reducing readmissions but not more effective at reducing hospital LOS or mortality. There was very low quality evidence that it is more effective at improving HRQOL or patient satisfaction.
References
-
- Naylor MD, Aiken LH, Kurtzman ET, Olds DM, Hirschman KB. The care span: the importance of transitional care in achieving health reform. 2011;30(4):746–54. Health Aff. - PubMed
-
- Holland DE, Harris MR. Discharge planning, transitional care, coordination of care and continuity of care: clarifying concepts and terms from the hospital perspective. 2007;26(4):3–19. Home Health Care Serv Q. - PubMed
-
- Samuels-Kalow ME, Stack AM, Porter SC. Effective discharge communication in the emergency department. Forthcoming. 2012 Ann Emerg Med. - PubMed
-
- Shepperd S, McClaran J, Phillips CO, Lannin NA, Clemson LM, McCluskey A, et al. Discharge planning from hospital to home. 2010 Mar;(1) Cochrane Database Sys Re. CD000313. - PubMed
-
- Guyatt GH, Oxman AD, Shunemann HJ, Tugwell P, Knottnerus A. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. 2011;64(4):380–2. Clin Epidemiol. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical