

Infant growth outcomes after maternal tenofovir disoproxil fumarate use during pregnancy
- PMID: 24169122
- PMCID: PMC3818710
- DOI: 10.1097/QAI.0b013e3182a7adb2
Infant growth outcomes after maternal tenofovir disoproxil fumarate use during pregnancy
Abstract
Objective: To determine whether maternal use of tenofovir disoproxil fumarate for treatment of HIV in pregnancy predicts fetal and infant growth.
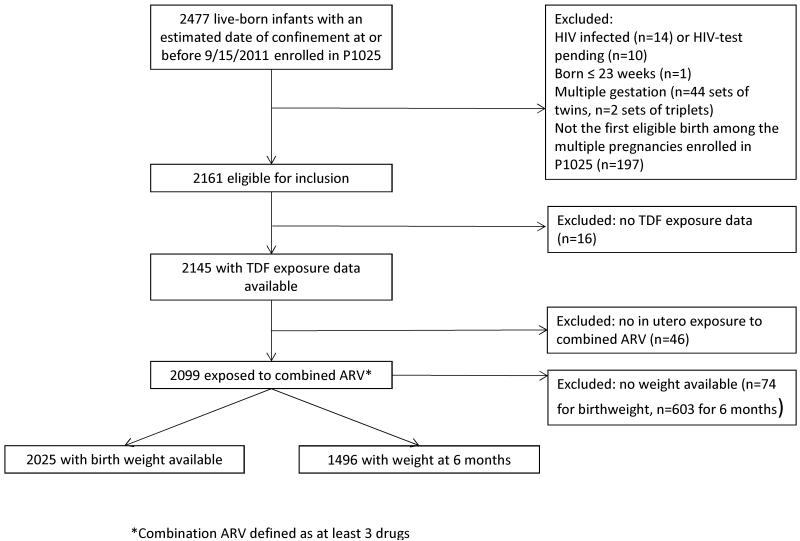
Methods: The study population included HIV-uninfected live-born singleton infants of mothers enrolled in the International Maternal Pediatric Adolescent AIDS Clinical Trials Group protocol P1025 (born 2002-2011) in the United States and exposed in utero to a combined (triple or more) antiretroviral regimen. Infant weight at birth and 6 months was compared between infants exposed and unexposed to tenofovir in utero using 2-sample t test, χ test, and multivariable linear and logistic regression models, including demographic and maternal characteristics.
Results: Among 2025 infants with measured birth weight, there was no difference between those exposed (N = 630, 31%) versus unexposed to tenofovir in mean birth weight (2.75 vs. 2.77 kg, P = 0.64) or mean gestational age- and sex-adjusted birth weight z-score (WASZ) (0.14 vs. 0.14, P = 0.90). Among 1496 infants followed for 6 months, there was no difference in mean weight at 6 months between tenofovir-exposed (N = 457, 31%) and tenofovir-unexposed infants (7.64 vs. 7.59 kg, P = 0.52) or in mean WASZ (0.29 vs. 0.26, P = 0.61). Tenofovir exposure during the second/third trimester, relative to no exposure, significantly predicted underweight (WASZ < 5%) at age 6 months [odds ratio (95% confidence interval): 2.06 (1.01 to 3.95), P = 0.04]. Duration of tenofovir exposure did not predict neonatal or infant growth.
Conclusions: By most measures, in utero exposure to tenofovir did not significantly predict infant birth weight or growth through 6 months of age.
References
-
- Mother-to-child transmission of HIV infection in the era of highly active antiretroviral therapy. Clin Infect Dis. 2005 Feb 1;40(3):458–465. - PubMed
-
- Cooper ER, Charurat M, Mofenson L, et al. Combination antiretroviral strategies for the treatment of pregnant HIV-1-infected women and prevention of perinatal HIV-1 transmission. J Acquir Immune Defic Syndr. 2002 Apr 15;29(5):484–494. - PubMed
-
- [Accessed 4/10/13];Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission. Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States. 2012 Jul 31; http://aidsinfo.nih.gov/ContentFiles/PerinatalGL.pdf.
-
- World Health Organization [Accessed 3/08/13];ANTIRETROVIRAL DRUGS FOR TREATING PREGNANT WOMEN AND PREVENTING HIV INFECTION IN INFANTS: Recommendations for a public health approach-2010 version. 2010. http://whqlibdoc.who.int/publications/2010/9789241599818_eng.pdf. - PubMed
-
- Guidelines for the use of antiretroviral agents in HIV-1-Infected adults and adolescents. http://aidsinfo.nih.gov/guidelines. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN267200800001G/DK/NIDDK NIH HHS/United States
- U01 AI068632/AI/NIAID NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- U01 AI068616/AI/NIAID NIH HHS/United States
- HHSN267200800001C/HD/NICHD NIH HHS/United States
- U01 AI041110/AI/NIAID NIH HHS/United States
- UM1 AI068616/AI/NIAID NIH HHS/United States
- UL1 TR001082/TR/NCATS NIH HHS/United States
- UL1 TR000038/TR/NCATS NIH HHS/United States
- N01-DK-9-001/DK/NIDDK NIH HHS/United States
- UL1 TR000154/TR/NCATS NIH HHS/United States
- UL1 TR000161/TR/NCATS NIH HHS/United States
- UM1 AI068632/AI/NIAID NIH HHS/United States
- 1 U01 AI068616/AI/NIAID NIH HHS/United States
- 5 U01 AI41110/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
