

Tumour-infiltrating lymphocytes predict for outcome in HPV-positive oropharyngeal cancer
- PMID: 24169344
- PMCID: PMC3899750
- DOI: 10.1038/bjc.2013.639
Tumour-infiltrating lymphocytes predict for outcome in HPV-positive oropharyngeal cancer
Abstract
Background: Human papillomavirus (HPV)-positive oropharyngeal cancer (OPSCC) is associated with improved survival compared with HPV-negative disease. However, a minority of HPV-positive patients have poor prognosis. Currently, there is no generally accepted strategy for identifying these patients.
Methods: We retrospectively analysed 270 consecutively treated OPSCC patients from three centres for effects of clinical, pathological, immunological, and molecular features on disease mortality. We used Cox regression to examine associations between factors and OPSCC death, and developed a prognostic model for 3-year mortality using logistic regression analysis.
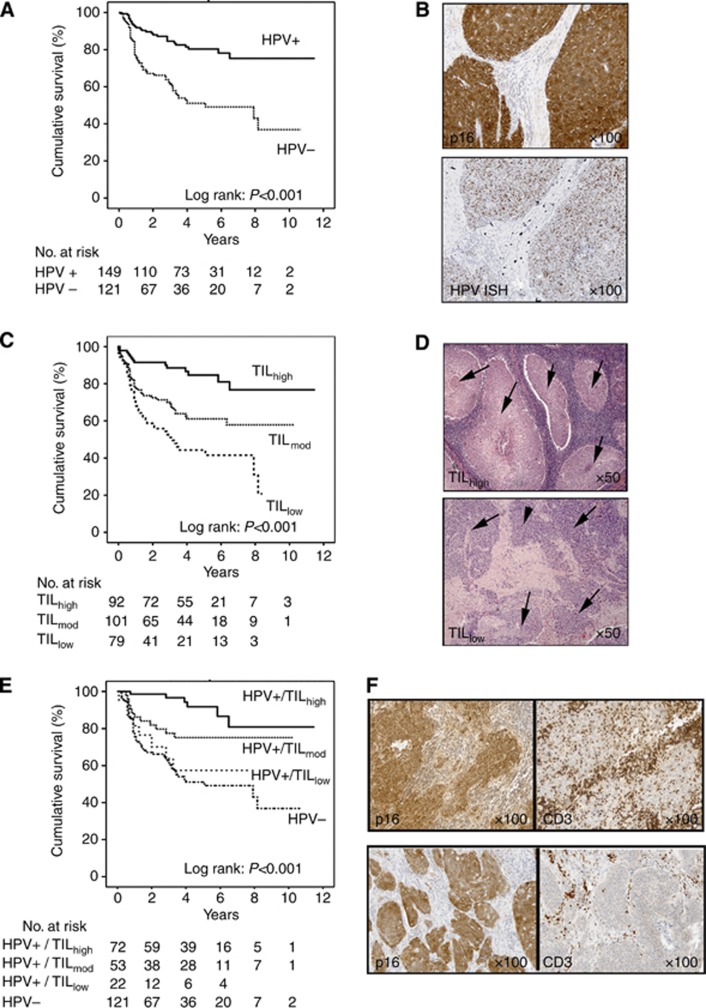
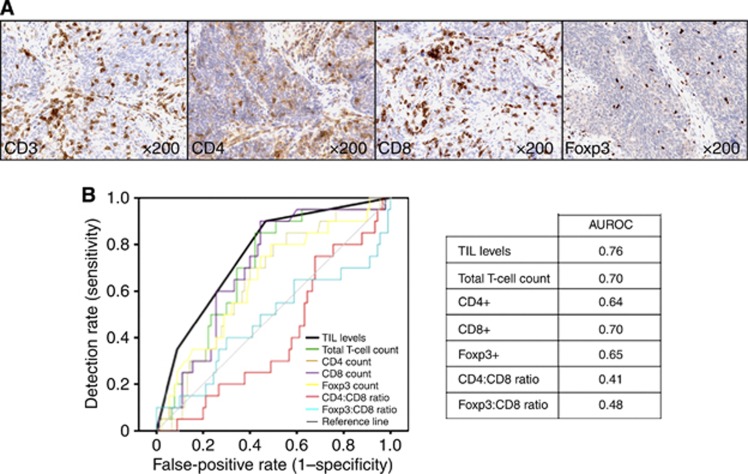
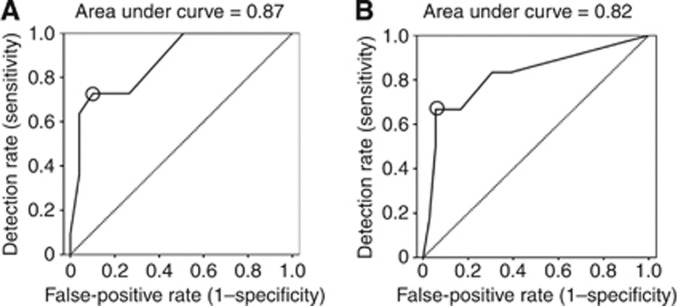
Results: Patients with HPV-positive tumours showed improved survival (hazard ratio (HR), 0.33 (0.21-0.53)). High levels of tumour-infiltrating lymphocytes (TILs) stratified HPV-positive patients into high-risk and low-risk groups (3-year survival; HPV-positive/TIL(high)=96%, HPV-positive/TIL(low)=59%). Survival of HPV-positive/TIL(low) patients did not differ from HPV-negative patients (HR, 1.01; P=0.98). We developed a prognostic model for HPV-positive tumours using a 'training' cohort from one centre; the combination of TIL levels, heavy smoking, and T-stage were significant (AUROC=0·87). This model was validated on patients from the other centres (detection rate 67%; false-positive rate 5.6%; AUROC=0·82).
Interpretation: Our data suggest that an immune response, reflected by TIL levels in the primary tumour, has an important role in the improved survival seen in most HPV-positive patients, and is relevant for the clinical evaluation of HPV-positive OPSCC.
Figures
Comment in
-
Tumour-infiltrating lymphocytes in the risk stratification of squamous cell carcinoma of the head and neck.Br J Cancer. 2014 Jan 21;110(2):269-70. doi: 10.1038/bjc.2013.746. Br J Cancer. 2014. PMID: 24448392 Free PMC article. No abstract available.
References
-
- Adelstein DJ, Ridge JA, Gillison ML, Chaturvedi AK, D'Souza G, Gravitt PE, Westra W, Psyrri A, Kast WM, Koutsky LA, Giuliano A, Krosnick S, Trotti A, Schuller DE, Forastiere A, Ullmann CD. Head and neck squamous cell cancer and the human papillomavirus: summary of a National Cancer Institute State of the Science Meeting, November 9-10, 2008, Washington, D.C. Head Neck. 2009;31 (11:1393–1422. - PubMed
-
- Albers A, Abe K, Hunt J, Wang J, Lopez-Albaitero A, Schaefer C, Gooding W, Whiteside TL, Ferrone S, DeLeo A, Ferris RL. Antitumor activity of human papillomavirus type 16 E7-specific T cells against virally infected squamous cell carcinoma of the head and neck. Cancer Res. 2005;65 (23:11146–11155. - PubMed
-
- Allison JE, Sakoda LC, Levin TR, Tucker JP, Tekawa IS, Cuff T, Pauly MP, Shlager L, Palitz AM, Zhao WK, Schwartz JS, Ransohoff DF, Selby JV. Screening for colorectal neoplasms with new fecal occult blood tests: update on performance characteristics. J Natl Cancer Inst. 2007;99 (19:1462–1470. - PubMed
-
- Badoual C, Hans S, Merillon N, Van Ryswick C, Ravel P, Benhamouda N, Levionnois E, Nizard M, Si-Mohamed A, Besnier N, Gey A, Rotem-Yehudar R, Pere H, Tran T, Guerin CL, Chauvat A, Dransart E, Alanio C, Albert S, Barry B, Sandoval F, Quintin-Colonna F, Bruneval P, Fridman WH, Lemoine FM, Oudard S, Johannes L, Olive D, Brasnu D, Tartour E. PD-1-expressing tumor-infiltrating T cells are a favorable prognostic biomarker in HPV-associated head and neck cancer. Cancer Res. 2013;73 (1:128–138. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
