

Cost-effectiveness of HIV treatment as prevention in serodiscordant couples
- PMID: 24171517
- PMCID: PMC3913536
- DOI: 10.1056/NEJMsa1214720
Cost-effectiveness of HIV treatment as prevention in serodiscordant couples
Abstract
Background: The cost-effectiveness of early antiretroviral therapy (ART) in persons infected with human immunodeficiency virus (HIV) in serodiscordant couples is not known. Using a computer simulation of the progression of HIV infection and data from the HIV Prevention Trials Network 052 study, we projected the cost-effectiveness of early ART for such persons.
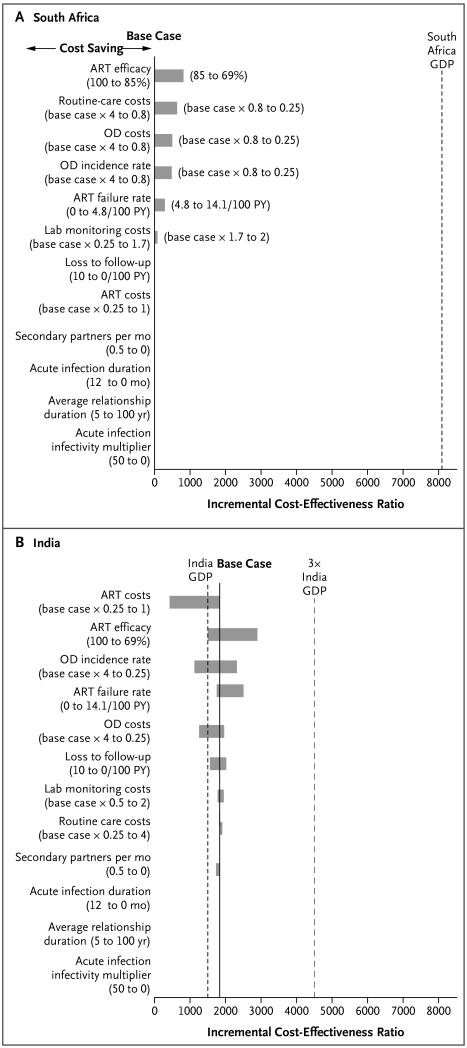
Methods: For HIV-infected partners in serodiscordant couples in South Africa and India, we compared the early initiation of ART with delayed ART. Five-year and lifetime outcomes included cumulative HIV transmissions, life-years, costs, and cost-effectiveness. We classified early ART as very cost-effective if its incremental cost-effectiveness ratio was less than the annual per capita gross domestic product (GDP; $8,100 in South Africa and $1,500 in India), as cost-effective if the ratio was less than three times the GDP, and as cost-saving if it resulted in a decrease in total costs and an increase in life-years, as compared with delayed ART.
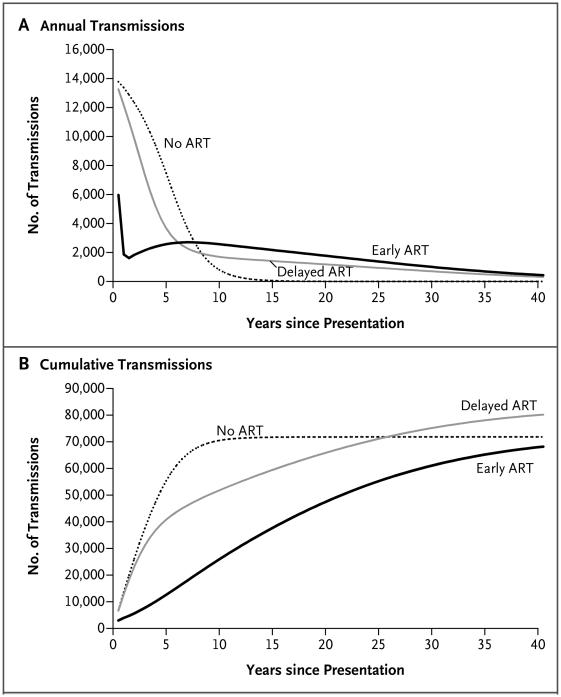
Results: In South Africa, early ART prevented opportunistic diseases and was cost-saving over a 5-year period; over a lifetime, it was very cost-effective ($590 per life-year saved). In India, early ART was cost-effective ($1,800 per life-year saved) over a 5-year period and very cost-effective ($530 per life-year saved) over a lifetime. In both countries, early ART prevented HIV transmission over short periods, but longer survival attenuated this effect; the main driver of life-years saved was a clinical benefit for treated patients. Early ART remained very cost-effective over a lifetime under most modeled assumptions in the two countries.
Conclusions: In South Africa, early ART was cost-saving over a 5-year period. In both South Africa and India, early ART was projected to be very cost-effective over a lifetime. With individual, public health, and economic benefits, there is a compelling case for early ART for serodiscordant couples in resource-limited settings. (Funded by the National Institute of Allergy and Infectious Diseases and others.).
Figures
Comment in
-
Cost-effectiveness of HIV treatment as prevention in serodiscordant couples.N Engl J Med. 2014 Feb 6;370(6):581-2. doi: 10.1056/NEJMc1314998. N Engl J Med. 2014. PMID: 24499229 No abstract available.
-
Cost-effectiveness of HIV treatment as prevention in serodiscordant couples.N Engl J Med. 2014 Feb 6;370(6):581. doi: 10.1056/NEJMc1314998. N Engl J Med. 2014. PMID: 24499230 No abstract available.
References
-
- Grinsztejn B, Hosseinipour M, Swindells S, et al. Proceedings of the XIX International AIDS Conference. Washington, DC: Jul 21-27, 2012. Effect of early versus delayed initiation of antiretroviral therapy (ART) on clinical outcomes in the HPTN 052 randomized clinical trial. abstract.
Publication types
MeSH terms
Substances
Grants and funding
- U01-AI068617/AI/NIAID NIH HHS/United States
- U01-AI068619/AI/NIAID NIH HHS/United States
- U01 AI068617/AI/NIAID NIH HHS/United States
- UM1 AI068613/AI/NIAID NIH HHS/United States
- R01 AI058736/AI/NIAID NIH HHS/United States
- UM1-AI068613/AI/NIAID NIH HHS/United States
- U01-AI068613/AI/NIAID NIH HHS/United States
- R01 MH087328/MH/NIMH NIH HHS/United States
- U01 AI068619/AI/NIAID NIH HHS/United States
- UM1-AI068619/AI/NIAID NIH HHS/United States
- P30 MH062294/MH/NIMH NIH HHS/United States
- R01 AI093269/AI/NIAID NIH HHS/United States
- U01 AI068613/AI/NIAID NIH HHS/United States
- UM1 AI068619/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
- UM1-AI068617/AI/NIAID NIH HHS/United States
- UM1 AI068617/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical