

Treating lateral epicondylitis with corticosteroid injections or non-electrotherapeutical physiotherapy: a systematic review
- PMID: 24171937
- PMCID: PMC3816235
- DOI: 10.1136/bmjopen-2013-003564
Treating lateral epicondylitis with corticosteroid injections or non-electrotherapeutical physiotherapy: a systematic review
Abstract
Objectives: To evaluate the current evidence for the efficacy of corticosteroid injection and non-electrotherapeutic physiotherapy compared with control for treating lateral epicondylitis.
Design: Systematic review.
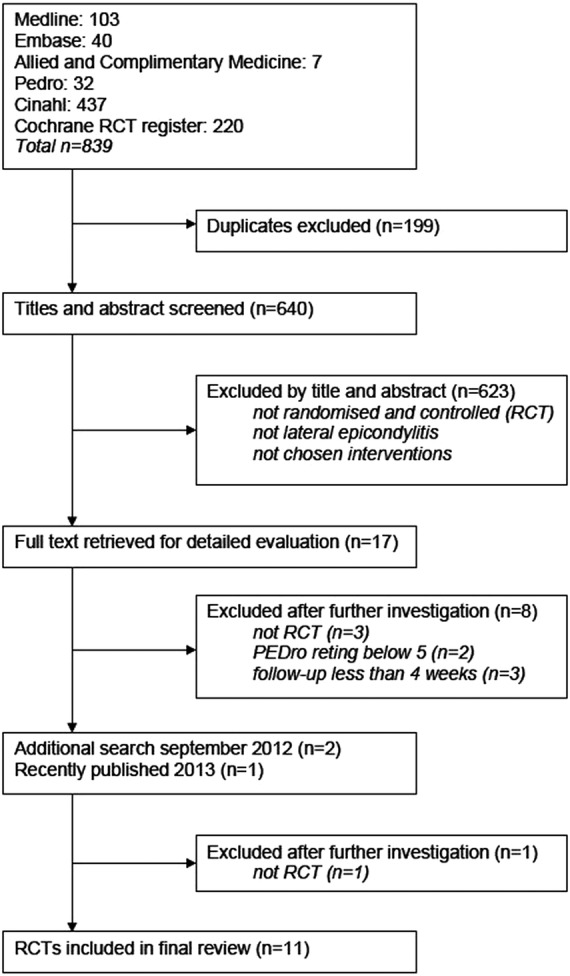
Participants: We searched five databases in September 2012 for randomised controlled studies with a minimum quality rating. Of the 640 studies retrieved, 11 were included, representing 1161 patients of both sexes and all ages.
Interventions: Corticosteroid injection and non-electrotherapeutic physiotherapy.
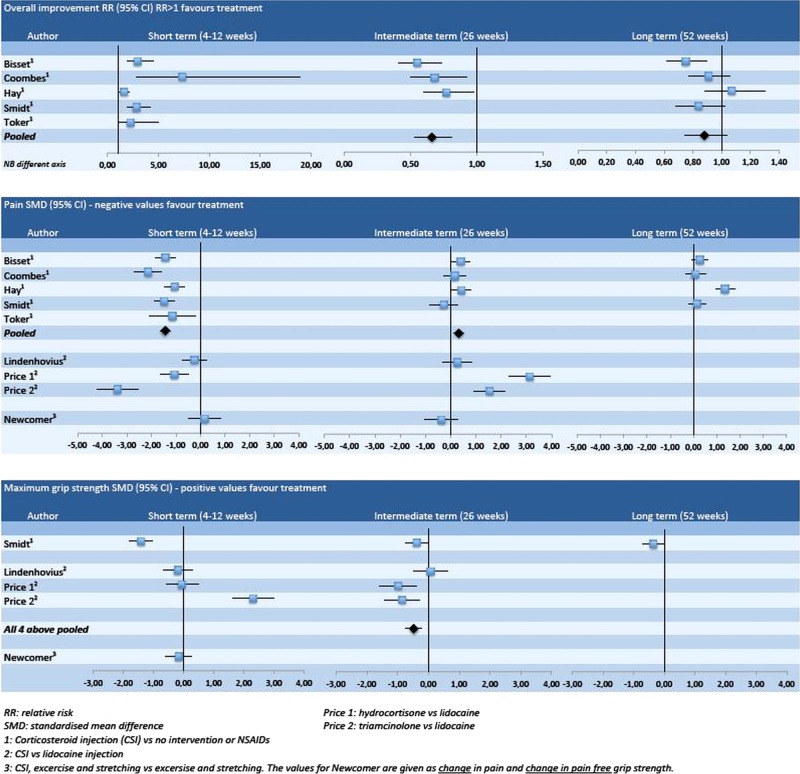
Outcome measures: Relative risk (RR) or standardised mean difference (SMD) for overall improvement, pain and grip strength at 4-12, 26 and 52 weeks of follow-up.
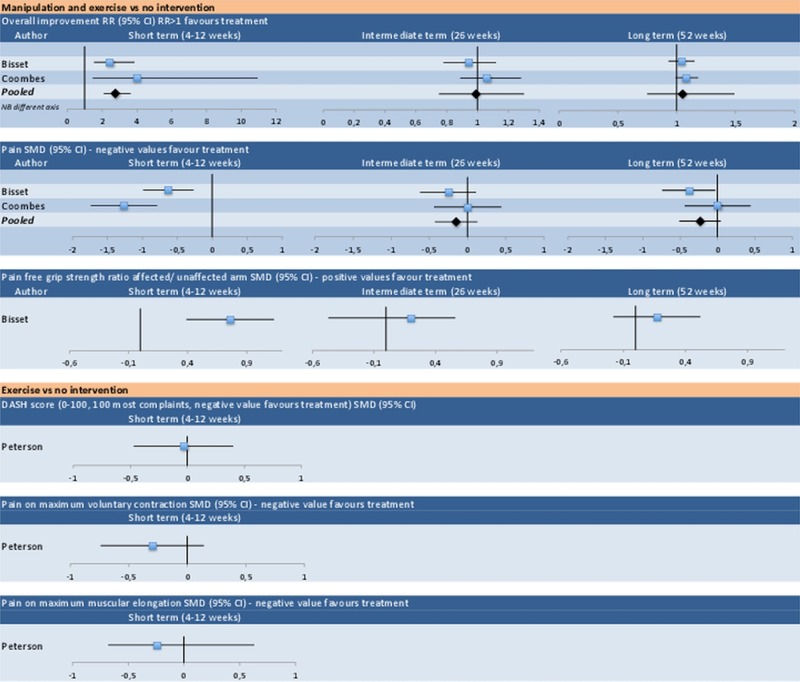
Results: Corticosteroid injection gave a short-term reduction in pain versus no intervention or non-steroidal anti-inflammatory drugs (SMD -1.43, 95% CI -1.64 to -1.23). At intermediate follow-up, we found an increase in pain (SMD 0.32, 95% CI 0.13 to 0.51), reduction in grip strength (SMD -0.48, 95% CI -0.73 to -0.24) and negative effect on the overall improvement effect (RR 0.66 (0.53 to 0.81)). For corticosteroid injection versus lidocaine injection, the evidence was conflicting. At long-term follow-up, there was no difference on overall improvement and grip strength, with conflicting evidence for pain. Manipulation and exercise versus no intervention showed beneficial effect at short-term follow-up (overall improvement RR 2.75, 95% CI 1.30 to 5.82), but no significant difference at intermediate or long-term follow-up. We found moderate evidence for short-term and long-term effects of eccentric exercise and stretching versus no intervention. For exercise versus no intervention and eccentric or concentric exercise and stretching versus stretching alone, we found moderate evidence of no short-term effect.
Conclusions: Corticosteroid injections have a short-term beneficial effect on lateral epicondylitis, but a negative effect in the intermediate term. Evidence on the long-term effect is conflicting. Manipulation and exercise and exercise and stretching have a short-term effect, with the latter also having a long-term effect.
Keywords: SPORTS MEDICINE.
Figures

Similar articles
-
Corticosteroid or placebo injection combined with deep transverse friction massage, Mills manipulation, stretching and eccentric exercise for acute lateral epicondylitis: a randomised, controlled trial.BMC Musculoskelet Disord. 2015 May 20;16:122. doi: 10.1186/s12891-015-0582-6. BMC Musculoskelet Disord. 2015. PMID: 25989985 Free PMC article. Clinical Trial.
-
Corticosteroid and other injections in the management of tendinopathies: a review.Clin J Sport Med. 2011 Nov;21(6):540-1. doi: 10.1097/01.jsm.0000407929.35973.b9. Clin J Sport Med. 2011. PMID: 22064721
-
Behavioural modification interventions for medically unexplained symptoms in primary care: systematic reviews and economic evaluation.Health Technol Assess. 2020 Sep;24(46):1-490. doi: 10.3310/hta24460. Health Technol Assess. 2020. PMID: 32975190 Free PMC article.
-
Epidural corticosteroid injections for lumbosacral radicular pain.Cochrane Database Syst Rev. 2020 Apr 9;4(4):CD013577. doi: 10.1002/14651858.CD013577. Cochrane Database Syst Rev. 2020. PMID: 32271952 Free PMC article.
-
Manual Therapy and Exercise Have Similar Outcomes to Corticosteroid Injections in the Management of Patients With Subacromial Pain Syndrome: A Systematic Review and Meta-Analysis.Cureus. 2023 Nov 16;15(11):e48907. doi: 10.7759/cureus.48907. eCollection 2023 Nov. Cureus. 2023. PMID: 38111394 Free PMC article. Review.
Cited by
-
Corticosteroid or placebo injection combined with deep transverse friction massage, Mills manipulation, stretching and eccentric exercise for acute lateral epicondylitis: a randomised, controlled trial.BMC Musculoskelet Disord. 2015 May 20;16:122. doi: 10.1186/s12891-015-0582-6. BMC Musculoskelet Disord. 2015. PMID: 25989985 Free PMC article. Clinical Trial.
-
CORR Insights(®): A Randomized Trial Among Compression Plus Nonsteroidal Antiinflammatory Drugs, Aspiration, and Aspiration With Steroid Injection for Nonseptic Olecranon Bursitis.Clin Orthop Relat Res. 2016 Mar;474(3):784-6. doi: 10.1007/s11999-015-4608-z. Epub 2015 Oct 22. Clin Orthop Relat Res. 2016. PMID: 26493988 Free PMC article. No abstract available.
-
Management of tennis elbow: a survey of UK clinical practice.Shoulder Elbow. 2019 Jun;11(3):233-238. doi: 10.1177/1758573217738199. Epub 2017 Oct 25. Shoulder Elbow. 2019. PMID: 31210796 Free PMC article.
-
Novel Ultrasound-Guided Radiofrequency Ablation of the Epicondylar Branch of the Posterior Cutaneous Nerve of the Forearm for Recalcitrant Lateral Epicondylosis.Cureus. 2024 May 28;16(5):e61222. doi: 10.7759/cureus.61222. eCollection 2024 May. Cureus. 2024. PMID: 38939254 Free PMC article.
-
Comparison of local massage, steroid injection, and extracorporeal shock wave therapy efficacy in the treatment of lateral epicondylitis.Jt Dis Relat Surg. 2024 Apr 26;35(2):386-395. doi: 10.52312/jdrs.2024.1648. Epub 2024 Apr 26. Jt Dis Relat Surg. 2024. PMID: 38727119 Free PMC article. Clinical Trial.
References
-
- Chard MD, Hazleman BL. Tennis elbow—a reappraisal. Br J Rheumatol 1989;28:186–90 - PubMed
-
- Kivi P. The etiology and conservative treatment of humeral epicondylitis. Scand J Rehabil Med 1983;15:37–41 - PubMed
-
- Hudak PL, Cole DC, Haines AT. Understanding prognosis to improve rehabilitation: the example of lateral elbow pain. Arch Phys Med Rehabil 1996;77:586–93 - PubMed
-
- Murtagh J. Tennis elbow. Aust Fam Physician 1984;13:51. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources