

Issues in hypertriglyceridemic pancreatitis: an update
- PMID: 24172179
- PMCID: PMC3939000
- DOI: 10.1097/01.mcg.0000436438.60145.5a
Issues in hypertriglyceridemic pancreatitis: an update
Abstract
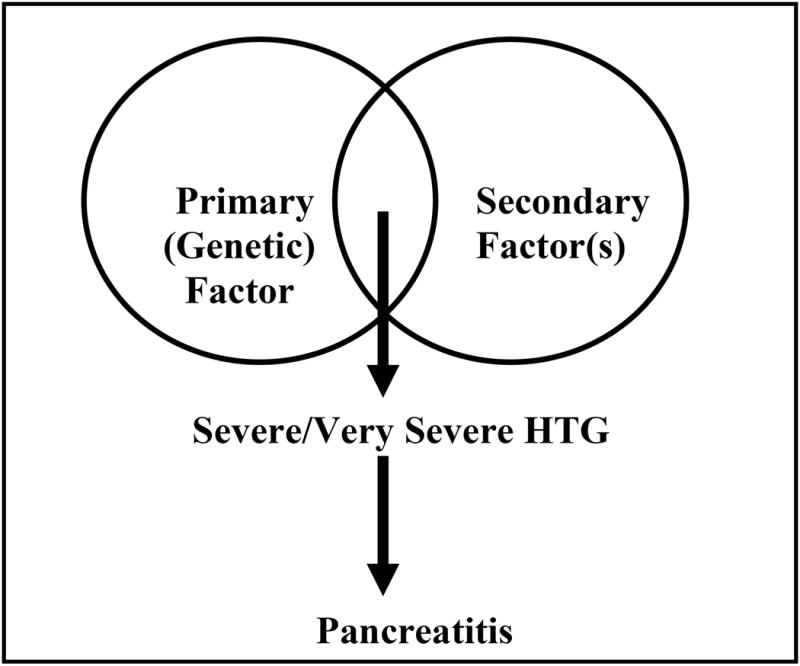
Hypertriglyceridemia (HTG) is a well-established but underestimated cause of acute pancreatitis and recurrent acute pancreatitis. The clinical presentation of HTG-induced pancreatitis (HTG pancreatitis) is similar to other causes. Pancreatitis secondary to HTG is typically seen in the presence of one or more secondary factors (uncontrolled diabetes, alcoholism, medications, pregnancy) in a patient with an underlying common genetic abnormality of lipoprotein metabolism (familial combined hyperlipidemia or familial HTG). Less commonly, a patient with rare genetic abnormality (familial chylomicronemic syndrome) with or without an additional secondary factor is encountered. The risk of acute pancreatitis in patients with serum triglycerides >1000 and >2000 mg/dL is ∼ 5% and 10% to 20%, respectively. It is not clear whether HTG pancreatitis is more severe than when it is due to other causes. Clinical management of HTG pancreatitis is similar to that of other causes. Insulin infusion in diabetic patients with HTG can rapidly reduce triglyceride (TG) levels. Use of apheresis is still experimental and better designed studies are needed to clarify its role in the management of HTG pancreatitis. Diet, lifestyle changes, and control of secondary factors are key to the treatment, and medications are useful adjuncts to the long-term management of TG levels. Control of TG levels to 500 mg/dL or less can effectively prevent recurrences of pancreatitis.
Conflict of interest statement
Figures
References
-
- Yadav D, Pitchumoni CS. Issues in hyperlipidemic pancreatitis. J Clin Gastroenterol. 2003;36:54–62. - PubMed
-
- Dominguez-Munoz JE, Malfertheiner P, Ditschuneit HH, et al. Hyperlipidemia in acute pancreatitis. Relationship with etiology, onset, and severity of the disease. Int J Pancreatol. 1991;10:261–7. - PubMed
-
- Balachandra S, Virlos IT, King NK, et al. Hyperlipidaemia and outcome in acute pancreatitis. Int J Clin Pract. 2006;60:156–9. - PubMed
-
- Fortson MR, Freedman SN, Webster PD., 3rd Clinical assessment of hyperlipidemic pancreatitis. Am J Gastroenterol. 1995;90:2134–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
