

Exercise training improves endothelial function in resistance arteries of young prehypertensives
- PMID: 24172292
- PMCID: PMC4159938
- DOI: 10.1038/jhh.2013.109
Exercise training improves endothelial function in resistance arteries of young prehypertensives
Abstract
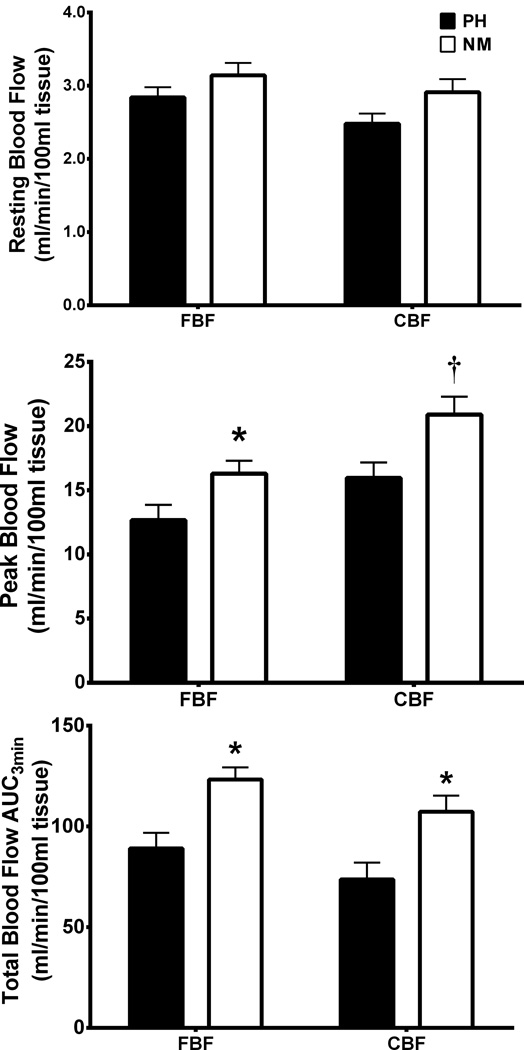
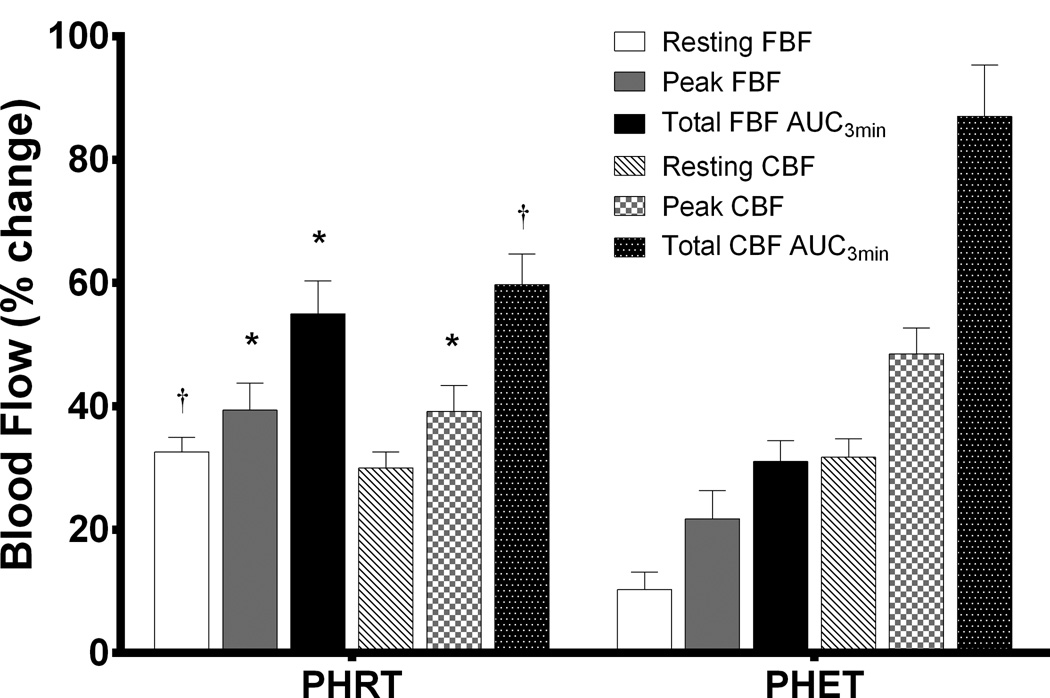
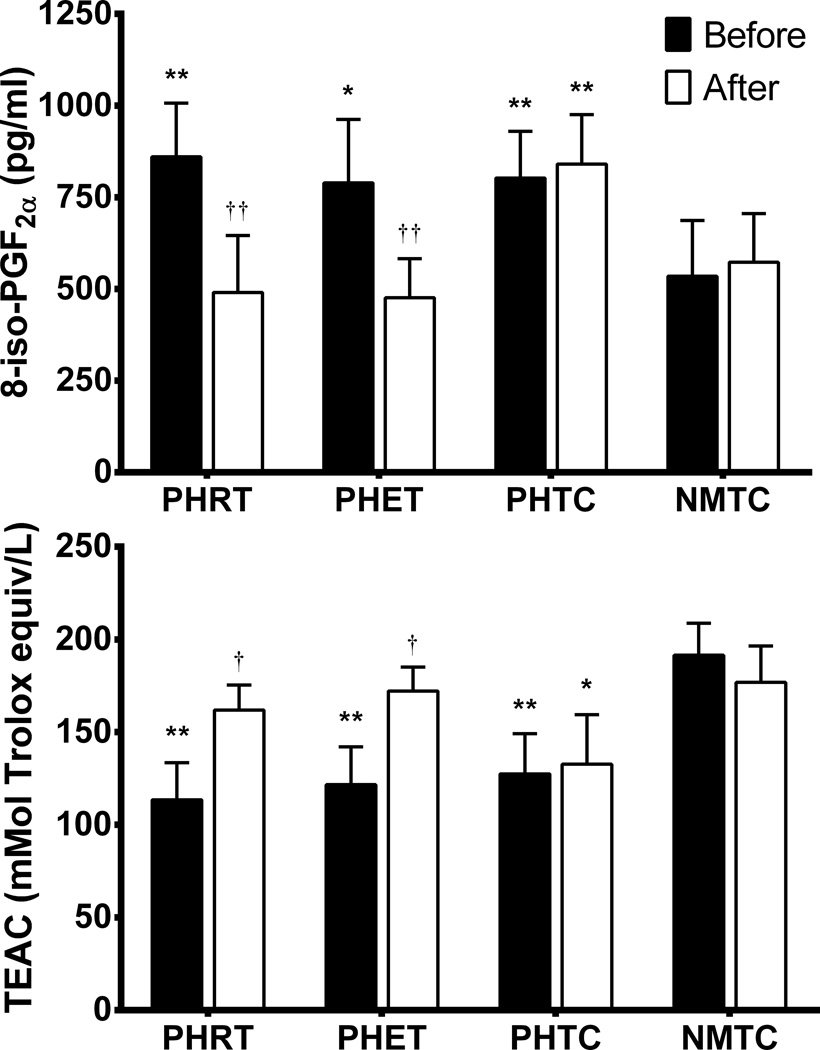
Prehypertension is associated with reduced conduit artery endothelial function and perturbation of oxidant/antioxidant status. It is unknown whether endothelial dysfunction persists to resistance arteries and whether exercise training affects oxidant/antioxidant balance in young prehypertensives. We examined resistance artery function using venous occlusion plethysmography measurement of forearm (FBF) and calf blood flow (CBF) at rest and during reactive hyperaemia (RH), as well as lipid peroxidation (8-iso-PGF2α) and antioxidant capacity (Trolox-equivalent antioxidant capacity; TEAC) before and after exercise intervention or time control. Forty-three unmedicated prehypertensive and 15 matched normotensive time controls met screening requirements and participated in the study (age: 21.1±0.8 years). Prehypertensive subjects were randomly assigned to resistance exercise training (PHRT; n=15), endurance exercise training (PHET; n=13) or time-control groups (PHTC; n=15). Treatment groups exercised 3 days per week for 8 weeks. Peak and total FBF were lower in prehypertensives than normotensives (12.7±1.2 ml min(-1) per100 ml tissue and 89.1±7.7 ml min(-1) per 100 ml tissue vs 16.3±1.0 ml min(-1) per 100 ml tissue and 123.3±6.4 ml min(-1) per 100 ml tissue, respectively; P<0.05). Peak and total CBF were lower in prehypertensives than normotensives (15.3±1.2 ml min(-1) per 100 ml tissue and 74±8.3 ml min(-1) per 100 ml tissue vs 20.9±1.4 ml min(-1) per 100 ml tissue and 107±9.2 ml min(-1) per 100 ml tissue, respectively; P<0.05). PHRT and PHET improved humoral measures of TEAC (+24 and +30%) and 8-iso-PGF2α (-43 and -40%, respectively; P < or = 0.05). This study provides evidence that young prehypertensives exhibit reduced resistance artery endothelial function and that short-term (8 weeks) resistance or endurance training are effective in improving resistance artery endothelial function and oxidant/antioxidant balance in young prehypertensives.
Conflict of interest statement
Figures
References
-
- Greenlund KJ, Croft JB, Mensah GA. Prevalence of heart disease and stroke risk factors in persons with prehypertension in the United States, 1999–2000. Arch Intern Med. 2004;164:2113–2118. - PubMed
-
- Chobanian AV. Prehypertension revisited. Hypertension. 2006;48:812–814. - PubMed
-
- Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, et al. Heart disease and stroke statistics--2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:480–486. - PubMed
-
- Giannotti G, Doerries C, Mocharla PS, Mueller MF, Bahlmann FH, Horvath T, et al. Impaired endothelial repair capacity of early endothelial progenitor cells in prehypertension: relation to endothelial dysfunction. Hypertension. 2010;55:1389–1397. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
