

Validation of noninvasive indices of global systolic function in patients with normal and abnormal loading conditions: a simultaneous echocardiography pressure-volume catheterization study
- PMID: 24173273
- PMCID: PMC3935312
- DOI: 10.1161/CIRCIMAGING.113.000722
Validation of noninvasive indices of global systolic function in patients with normal and abnormal loading conditions: a simultaneous echocardiography pressure-volume catheterization study
Abstract
Background: Noninvasive indices based on Doppler echocardiography are increasingly used in clinical cardiovascular research to evaluate left ventricular global systolic chamber function. Our objectives were to clinically validate ultrasound-based methods of global systolic chamber function to account for differences between patients in conditions of abnormal load, and to assess their sensitivity to load confounders.
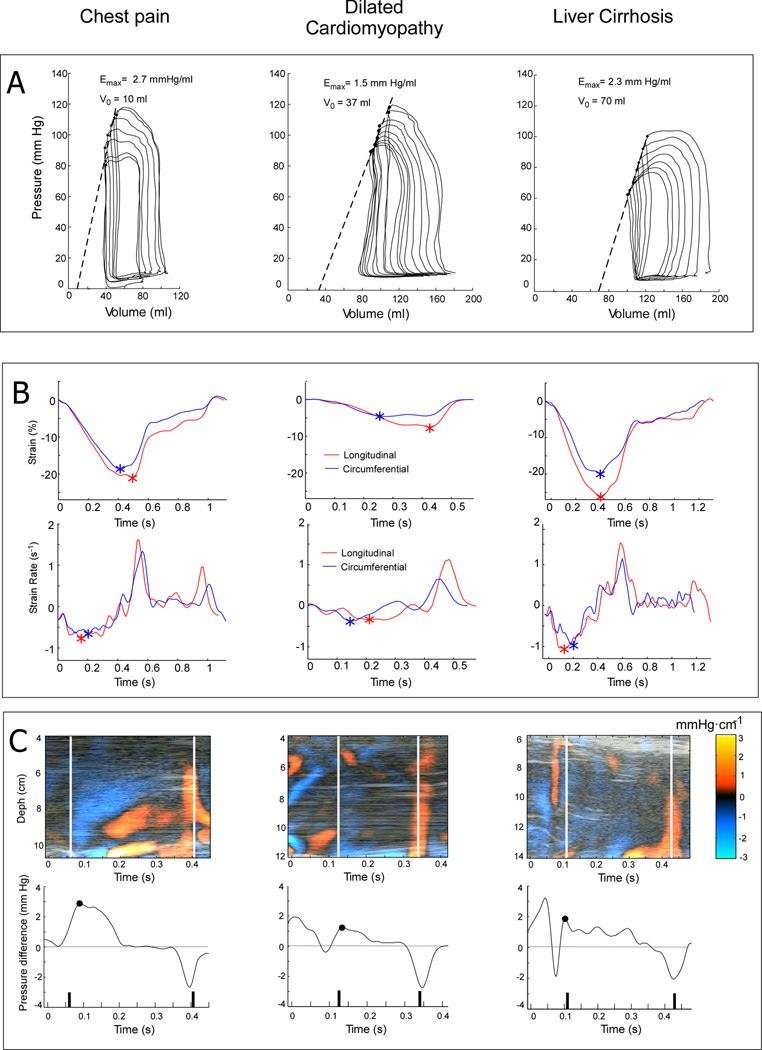
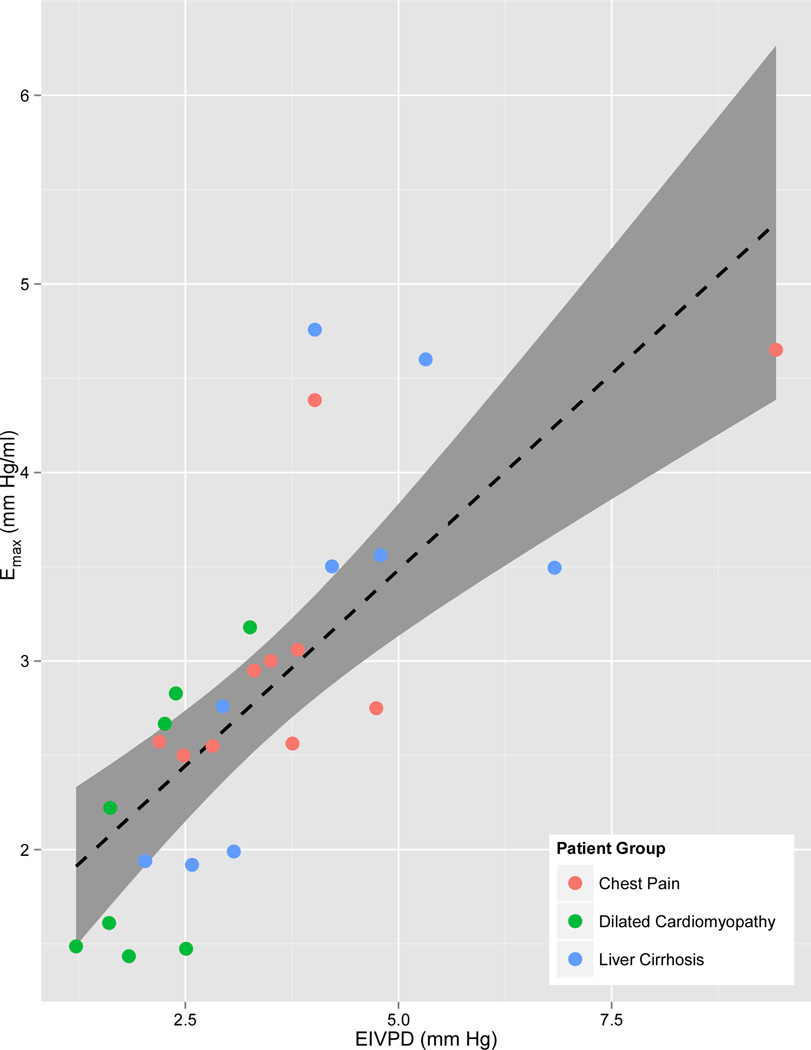
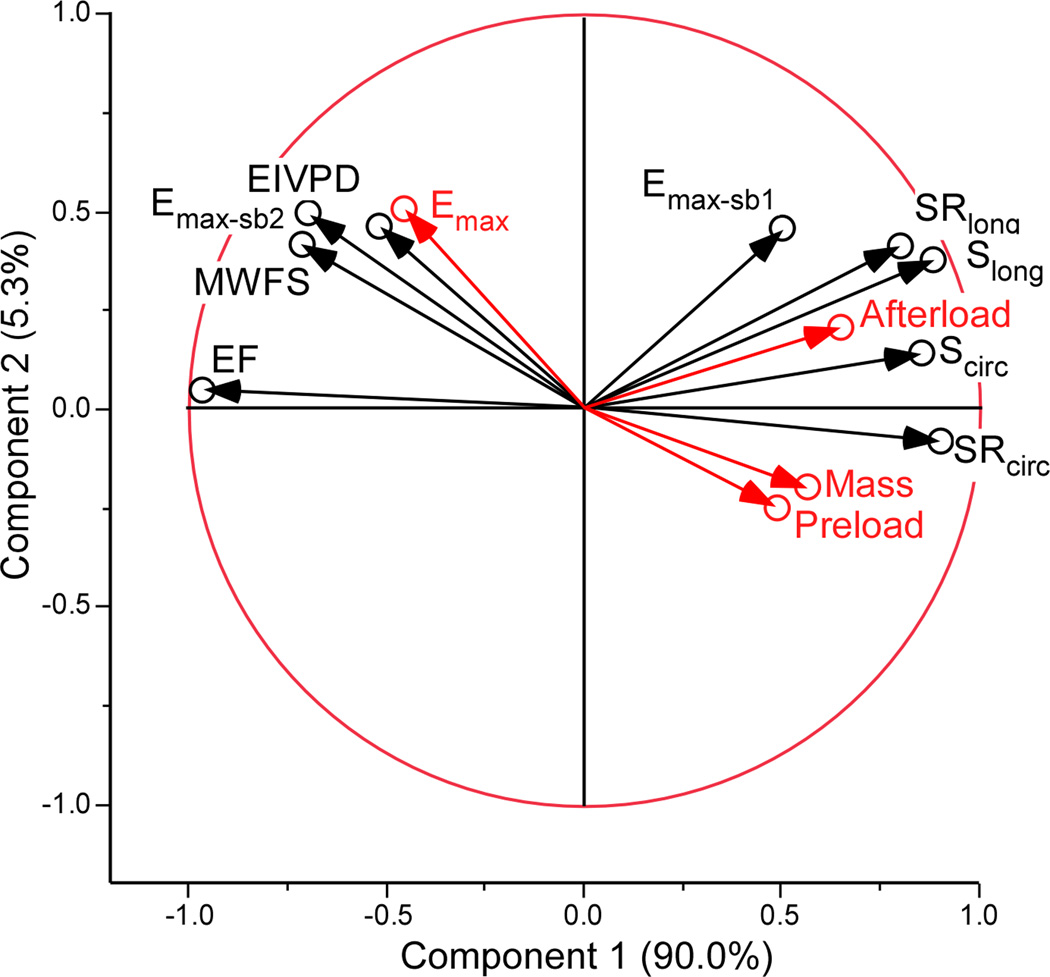
Methods and results: Twenty-seven patients (8 dilated cardiomyopathy, 10 normal ejection fraction, and 9 end-stage liver disease) underwent simultaneous echocardiography and left heart catheterization with pressure-conductance instrumentation. The reference index, maximal elastance (Emax), was calculated from pressure-volume loop data obtained during acute inferior vena cava occlusion. A wide range of values were observed for left ventricular systolic chamber function (Emax: 2.8±1.0 mm Hg/mL), preload, and afterload. Among the noninvasive indices tested, the peak ejection intraventricular pressure difference showed the best correlation with Emax (R=0.75). A significant but weaker correlation with Emax was observed for ejection fraction (R=0.41), midwall fractional shortening (R=0.51), global circumferential strain (R=-0.53), and strain rate (R=-0.46). Longitudinal strain and strain rate failed to correlate with Emax, as did noninvasive single-beat estimations of this index. Principal component and multiple regression analyses demonstrated that peak ejection intraventricular pressure difference was less sensitive to load, whereas ejection fraction and longitudinal strain and strain rate were heavily influenced by afterload.
Conclusions: Current ultrasound methods have limited accuracy to characterize global left ventricular systolic chamber function in a given patient. The Doppler-derived peak ejection intraventricular pressure difference should be preferred for this purpose because it best correlates with the reference index and is more robust in conditions of abnormal load.
Keywords: cardiac catheterization; echocardiography; hemodynamics; systole.
Figures
References
-
- Kosmala W, Jedrzejuk D, Derzhko R, Przewlocka-Kosmala M, Mysiak A, Bednarek-Tupikowska G. Left ventricular function impairment in patients with normal-weight obesity: contribution of abdominal fat deposition, profibrotic state, reduced insulin sensitivity, and proinflammatory activation. Circ Cardiovasc Imaging. 2012;5:349–356. - PubMed
-
- Steendijk P, Meliga E, Valgimigli M, Ten Cate FJ, Serruys PW. Acute effects of alcohol septal ablation on systolic and diastolic left ventricular function in patients with hypertrophic obstructive cardiomyopathy. Heart. 2008;94:1318–1322. - PubMed
-
- Yiu KH, Atsma DE, Delgado V, Ng AC, Witkowski TG, Ewe SH, Auger D, Holman ER, van Mil AM, Breuning MH, Tse HF, Bax JJ, Schalij MJ, Marsan NA. Myocardial structural alteration and systolic dysfunction in preclinical hypertrophic cardiomyopathy mutation carriers. PLoS One. 2012;7:e36115. - PMC - PubMed
-
- Sawaya H, Plana JC, Scherrer-Crosbie M. Newest echocardiographic techniques for the detection of cardiotoxicity and heart failure during chemotherapy. Heart Fail Clin. 2011;7:313–321. - PubMed
-
- Redfield MM, Jacobsen SJ, Borlaug BA, Rodeheffer RJ, Kass DA. Age- and gender-related ventricular-vascular stiffening: a community-based study. Circulation. 2005;112:2254–2262. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
