

The relationship between the survival of total knee arthroplasty and postoperative coronal, sagittal and rotational alignment of knee prosthesis
- PMID: 24173677
- PMCID: PMC3923934
- DOI: 10.1007/s00264-013-2097-9
The relationship between the survival of total knee arthroplasty and postoperative coronal, sagittal and rotational alignment of knee prosthesis
Abstract
Purpose: Our study sought to address four issues: (1) the relationship between postoperative overall anatomical knee alignment and the survival of total knee prostheses; (2) the relationship between postoperative coronal alignment of the femoral and tibial component and implant survival; (3) the relationship between postoperative sagittal alignment of the femoral and tibial components and implant survival; and (4) the relationship between postoperative rotational alignment of the femoral and tibial component and implant survival.
Methods: We reviewed 1,696 consecutive patients (3,048 knees). Radiographic and computed tomographic examinations were performed to determine the alignment of the femoral and tibial components. The mean duration of follow-up was 15.8 years (range, 11-18 years).
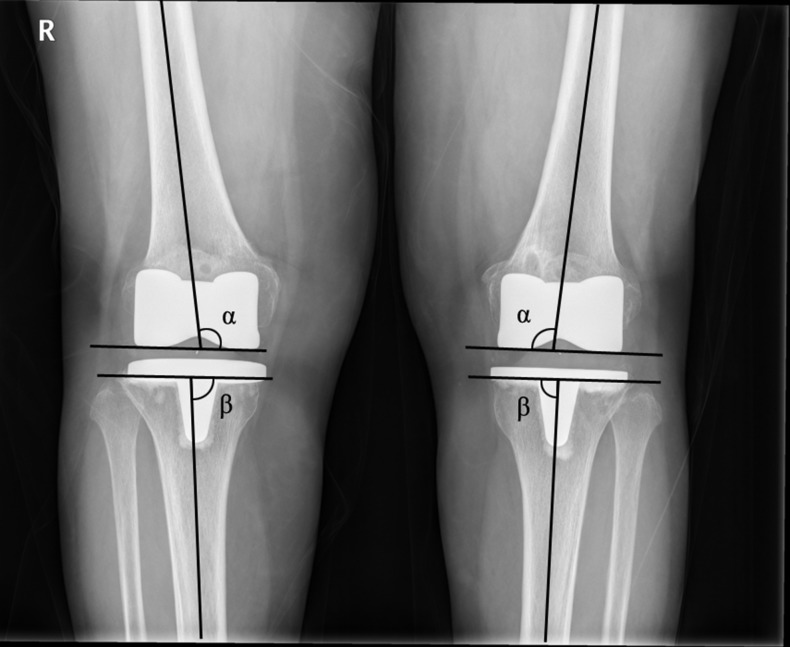
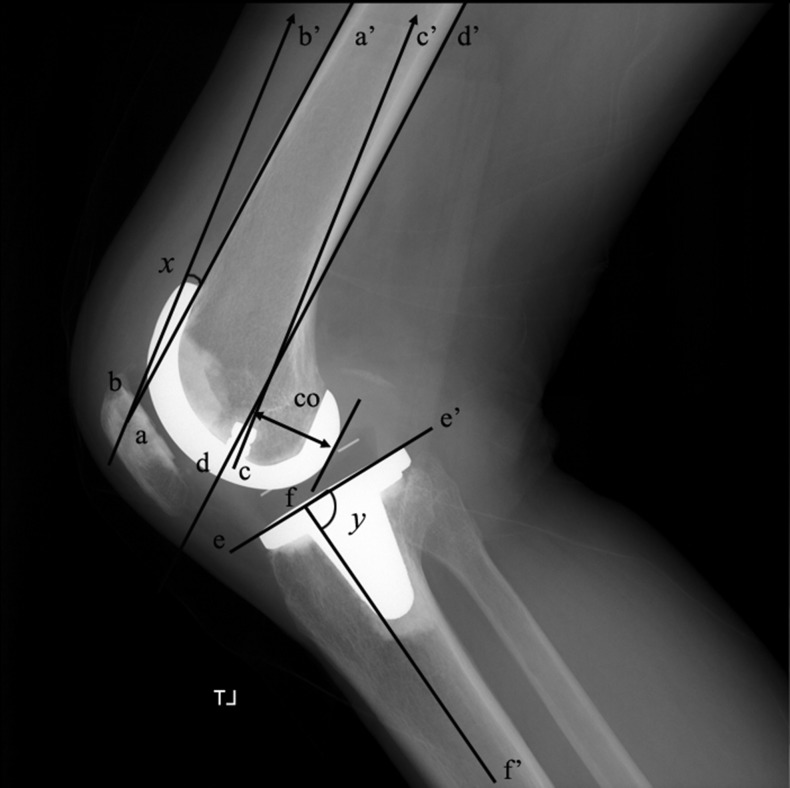
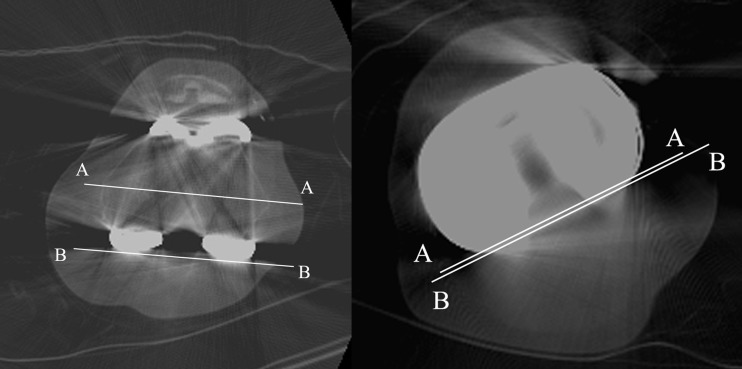
Results: Thirty (1.0%) of the 3,048 total knee arthroplasties failed for a reason other than infection and periprosthetic fracture. Risk factors for failure of the components were: overall anatomical knee alignment less than 3° valgus, coronal alignment of the femoral component less than 2.0° valgus, flexion of the femoral component greater than 3°, coronal alignment of the tibial component less than 90°, sagittal alignment of the tibial component less than 0° or greater than 7° slope, and external rotational alignment of the femoral and tibial components less than 2°
Conclusion: In order to improve the survival rate of the knee prosthesis, we believe that a surgeon should aim to place the total knee components in the position of: overall anatomical knee alignment at an angle of 3-7.5° valgus; femoral component alignment, 2-8.0° valgus; femoral sagittal alignment, 0-3°; tibial coronal alignment, 90°; tibial sagittal alignment, 0-7°; femoral rotational alignment, 2-5° external rotation; and tibial rotational alignment, 2-5° external rotation.
Figures
Similar articles
-
Can accuracy of component alignment be improved with Oxford UKA Microplasty® instrumentation?J Orthop Surg Res. 2020 Aug 26;15(1):354. doi: 10.1186/s13018-020-01868-3. J Orthop Surg Res. 2020. PMID: 32843044 Free PMC article.
-
Preoperative tibiofemoral rotational alignment is a risk factor for component rotational mismatch in total knee arthroplasty.Knee. 2021 Mar;29:448-456. doi: 10.1016/j.knee.2021.02.028. Epub 2021 Mar 17. Knee. 2021. PMID: 33743260
-
Rotational alignment of the tibial component affects the kinematic rotation of a weight-bearing knee after total knee arthroplasty.Knee. 2015 Jun;22(3):201-5. doi: 10.1016/j.knee.2015.01.002. Epub 2015 Jan 17. Knee. 2015. PMID: 25800285
-
What is the optimal alignment of the tibial and femoral components in knee arthroplasty?Acta Orthop. 2014 Sep;85(5):480-7. doi: 10.3109/17453674.2014.940573. Epub 2014 Jul 18. Acta Orthop. 2014. PMID: 25036719 Free PMC article. Review.
-
Efficacy Analysis of Selection of Distal Reference Point for Tibial Coronal Plane Osteotomy during Total Knee Arthroplasty: A Literature Review.Orthop Surg. 2021 Jul;13(5):1682-1693. doi: 10.1111/os.13054. Epub 2021 Jun 17. Orthop Surg. 2021. PMID: 34142453 Free PMC article. Review.
Cited by
-
Tibial alignment technique and its influence on clinical and functional outcomes following total knee arthroplasty.J Clin Orthop Trauma. 2020 Jul;11(Suppl 4):S534-S538. doi: 10.1016/j.jcot.2020.04.023. Epub 2020 Apr 28. J Clin Orthop Trauma. 2020. PMID: 32774025 Free PMC article.
-
Measurement of proximal tibial morphology in northeast Chinese population based on three-dimensional reconstruction computer tomography.Medicine (Baltimore). 2019 Nov;98(45):e17508. doi: 10.1097/MD.0000000000017508. Medicine (Baltimore). 2019. PMID: 31702611 Free PMC article.
-
Current concept of kinematic alignment total knee arthroplasty and its derivatives.Bone Jt Open. 2022 May;3(5):390-397. doi: 10.1302/2633-1462.35.BJO-2022-0021.R2. Bone Jt Open. 2022. PMID: 35532356 Free PMC article.
-
Mid-Term Clinical and Radiological Results at a Tertiary Care Hospital in Türkiye: Is Residual Varus Really Important After Mechanically-Aligned Total Knee Arthroplasty?Cureus. 2023 Feb 16;15(2):e35066. doi: 10.7759/cureus.35066. eCollection 2023 Feb. Cureus. 2023. PMID: 36942192 Free PMC article.
-
Evaluation of double-high insert mid-term outcomes in cruciate-retaining medial-pivotal total knee arthroplasty - a propensity score-matched analysis with averaged 8-year follow-up.BMC Musculoskelet Disord. 2022 Jun 14;23(1):571. doi: 10.1186/s12891-022-05484-6. BMC Musculoskelet Disord. 2022. PMID: 35701774 Free PMC article.
References
-
- Jeffery RS, Morris RW, Denham RA. Coronal alignment after total knee replacement. J Bone Joint Surg Br. 1991;73(5):709–714. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
