

TERT promoter mutations are highly recurrent in SHH subgroup medulloblastoma
- PMID: 24174164
- PMCID: PMC3830749
- DOI: 10.1007/s00401-013-1198-2
TERT promoter mutations are highly recurrent in SHH subgroup medulloblastoma
Abstract
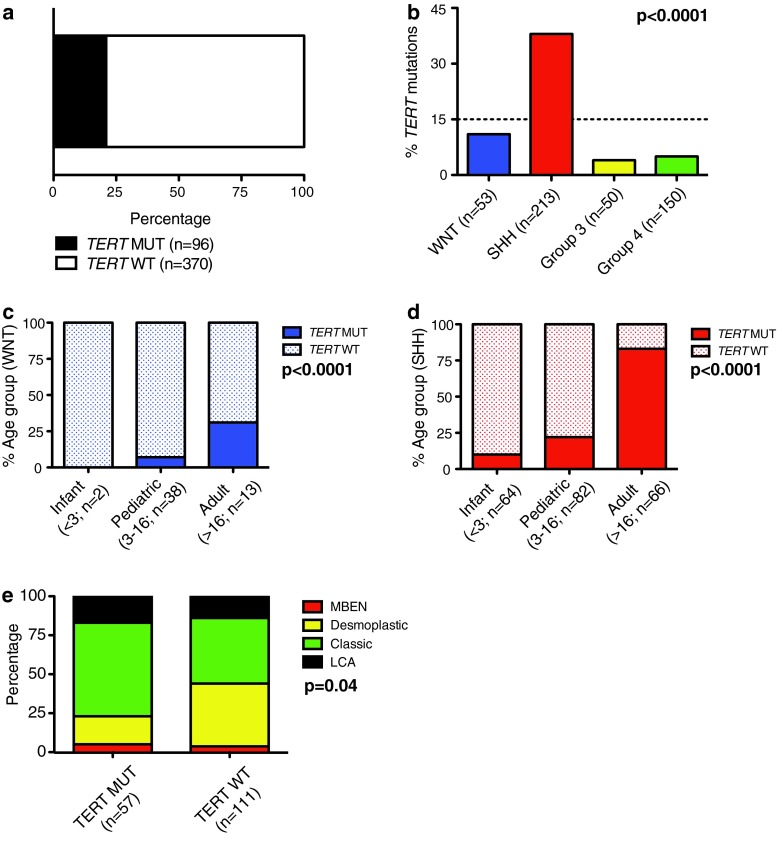
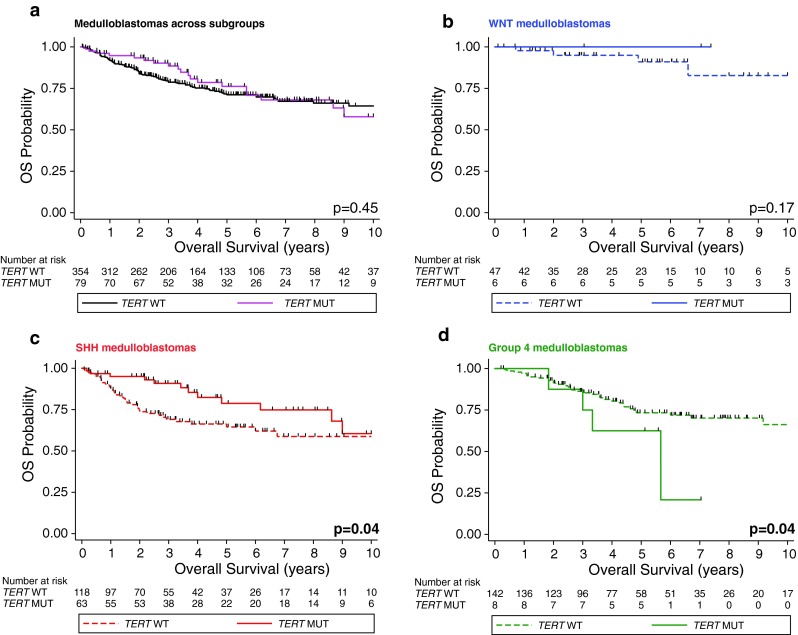
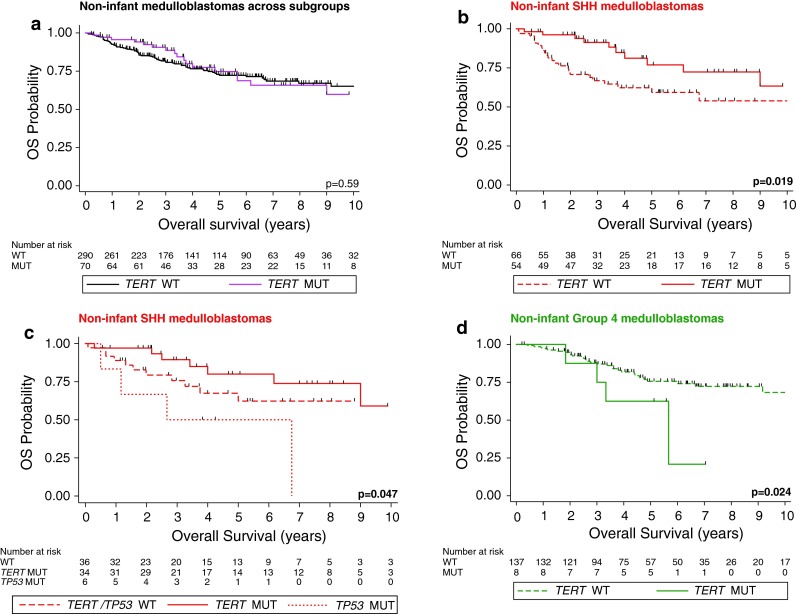
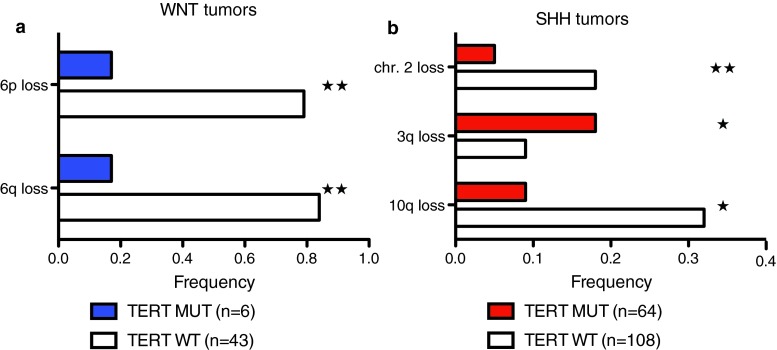
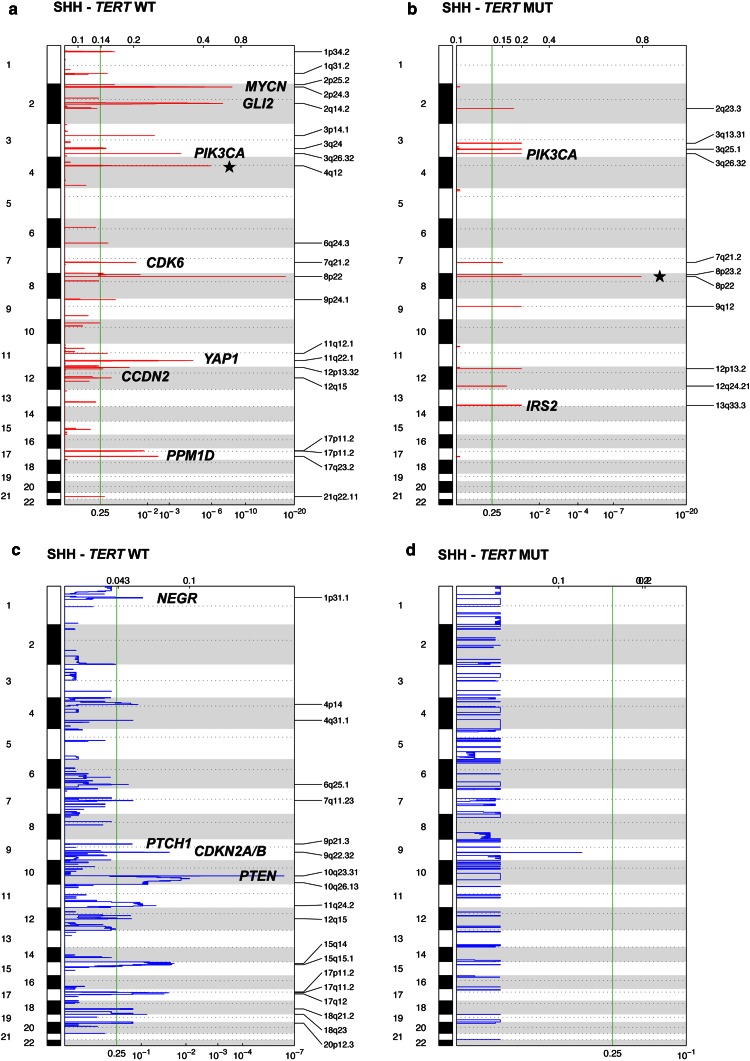
Telomerase reverse transcriptase (TERT) promoter mutations were recently shown to drive telomerase activity in various cancer types, including medulloblastoma. However, the clinical and biological implications of TERT mutations in medulloblastoma have not been described. Hence, we sought to describe these mutations and their impact in a subgroup-specific manner. We analyzed the TERT promoter by direct sequencing and genotyping in 466 medulloblastomas. The mutational distributions were determined according to subgroup affiliation, demographics, and clinical, prognostic, and molecular features. Integrated genomics approaches were used to identify specific somatic copy number alterations in TERT promoter-mutated and wild-type tumors. Overall, TERT promoter mutations were identified in 21 % of medulloblastomas. Strikingly, the highest frequencies of TERT mutations were observed in SHH (83 %; 55/66) and WNT (31 %; 4/13) medulloblastomas derived from adult patients. Group 3 and Group 4 harbored this alteration in <5 % of cases and showed no association with increased patient age. The prognostic implications of these mutations were highly subgroup-specific. TERT mutations identified a subset with good and poor prognosis in SHH and Group 4 tumors, respectively. Monosomy 6 was mostly restricted to WNT tumors without TERT mutations. Hallmark SHH focal copy number aberrations and chromosome 10q deletion were mutually exclusive with TERT mutations within SHH tumors. TERT promoter mutations are the most common recurrent somatic point mutation in medulloblastoma, and are very highly enriched in adult SHH and WNT tumors. TERT mutations define a subset of SHH medulloblastoma with distinct demographics, cytogenetics, and outcomes.
Figures
Comment in
-
Promoting a new brain tumor mutation: TERT promoter mutations in CNS tumors.Acta Neuropathol. 2013 Dec;126(6):789-92. doi: 10.1007/s00401-013-1207-5. Acta Neuropathol. 2013. PMID: 24217890 Free PMC article. No abstract available.
References
-
- Arita H, Narita Y, Fukushima S, Tateishi K, Matsushita Y, Yoshida A, Miyakita Y, Ohno M, Collins VP, Kawahara N, Shibui S, Ichimura K. Upregulating mutations in the TERT promoter commonly occur in adult malignant gliomas and are strongly associated with total 1p19q loss. Acta Neuropathol. 2013;126(2):267–276. doi: 10.1007/s00401-013-1141-6. - DOI - PubMed
-
- Castelo-Branco P, Choufani S, Mack S, Gallagher D, Zhang C, Lipman T, Zhukova N, Walker EJ, Martin D, Merino D, Wasserman JD, Elizabeth C, Alon N, Zhang L, Hovestadt V, Kool M, Jones DT, Zadeh G, Croul S, Hawkins C, Hitzler J, Wang JC, Baruchel S, Dirks PB, Malkin D, Pfister S, Taylor MD, Weksberg R, Tabori U. Methylation of the TERT promoter and risk stratification of childhood brain tumours: an integrative genomic and molecular study. Lancet Oncol. 2013;14(6):534–542. doi: 10.1016/S1470-2045(13)70110-4. - DOI - PubMed
-
- Cho YJ, Tsherniak A, Tamayo P, Santagata S, Ligon A, Greulich H, Berhoukim R, Amani V, Goumnerova L, Eberhart CG, Lau CC, Olson JM, Gilbertson RJ, Gajjar A, Delattre O, Kool M, Ligon K, Meyerson M, Mesirov JP, Pomeroy SL. Integrative genomic analysis of medulloblastoma identifies a molecular subgroup that drives poor clinical outcome. J Clin Oncol. 2011;29(11):1424–1430. doi: 10.1200/JCO.2010.28.5148. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
