

Human and viral interleukin-6 and other cytokines in Kaposi sarcoma herpesvirus-associated multicentric Castleman disease
- PMID: 24174627
- PMCID: PMC3868925
- DOI: 10.1182/blood-2013-08-519959
Human and viral interleukin-6 and other cytokines in Kaposi sarcoma herpesvirus-associated multicentric Castleman disease
Abstract
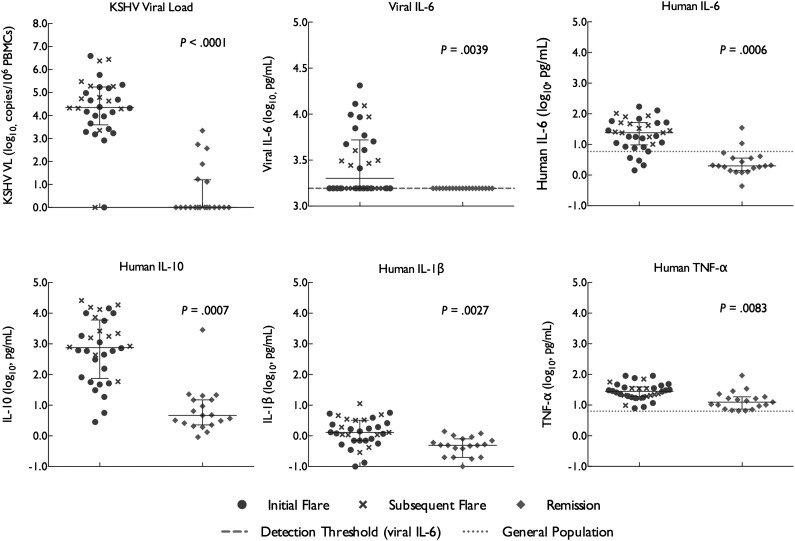
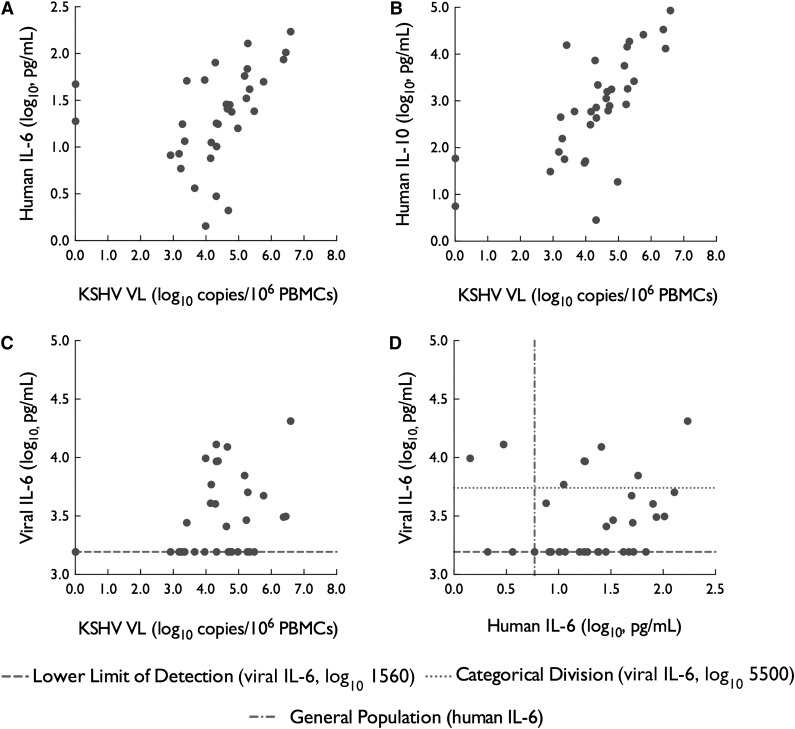
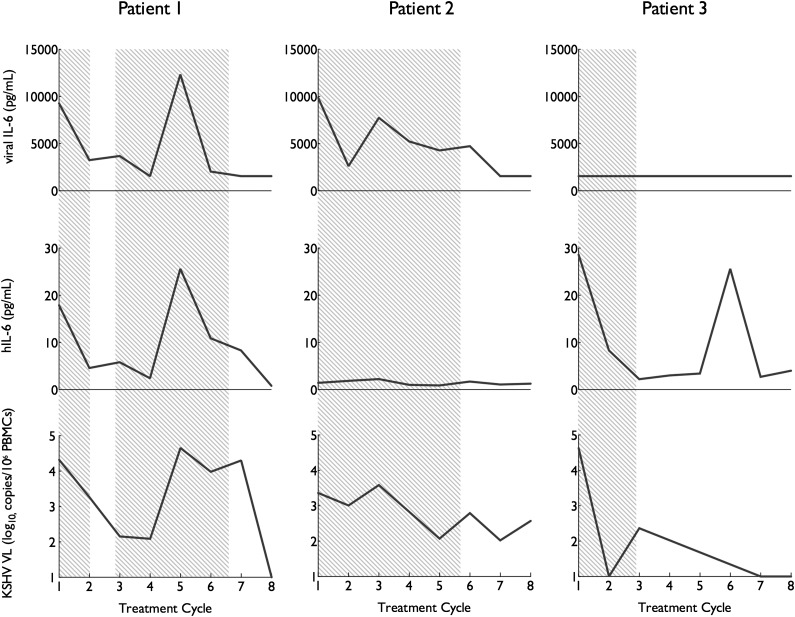
Kaposi sarcoma herpesvirus (KSHV)-associated multicentric Castleman disease (MCD) is a polyclonal B-cell lymphoproliferative disorder. Human (h) IL-6 and a KSHV-encoded homolog, viral IL-6, have been hypothesized to contribute to its pathogenesis, but their relative contributions to disease activity is not well understood. We prospectively characterized KSHV viral load (VL), viral (v) and hIL-6, and other cytokines during KSHV-MCD flare and remission in 21 patients with 34 flares and 20 remissions. KSHV-VL, vIL-6, hIL-6, IL-10, and to a lesser extent TNF-α, and IL-1β were each elevated during initial flares compared with remission. Flares fell into 3 distinct IL-6 profiles: those associated with elevations of vIL6-only (2 flares, 6%), hIL-6 elevations only (17 flares, 50%), and elevations in both hIL-6 and vIL-6 (13 flares, 38%). Compared with hIL-6-only flares, flares with elevated hIL-6 plus vIL-6 exhibited higher C-reactive protein (CRP) (P = .0009); worse hyponatremia (P = .02); higher KSHV VL (P = .016), and higher IL-10 (P = .012). This analysis shows vIL-6 and hIL-6 can independently or together lead to KSHV-MCD flares, and suggests that vIL-6 and hIL-6 may jointly contribute to disease severity. These findings have implications for the development of novel KSHV-MCD therapies targeting IL-6 and its downstream signaling. This trial was registered at clinicaltrials.gov as #NCT099073.
Trial registration: ClinicalTrials.gov NCT00092222 NCT00099073 NCT00092222.
Figures
References
-
- Castleman B, Iverson L, Menendez VP. Localized mediastinal lymphnode hyperplasia resembling thymoma. Cancer. 1956;9(4):822–830. - PubMed
-
- Keller AR, Hochholzer L, Castleman B. Hyaline-vascular and plasma-cell types of giant lymph node hyperplasia of the mediastinum and other locations. Cancer. 1972;29(3):670–683. - PubMed
-
- Frizzera G, Peterson BA, Bayrd ED, Goldman A. A systemic lymphoproliferative disorder with morphologic features of Castleman’s disease: clinical findings and clinicopathologic correlations in 15 patients. J Clin Oncol. 1985;3(9):1202–1216. - PubMed
-
- Yoshizaki K, Matsuda T, Nishimoto N, et al. Pathogenic significance of interleukin-6 (IL-6/BSF-2) in Castleman’s disease. Blood. 1989;74(4):1360–1367. - PubMed
-
- Soulier J, Grollet L, Oksenhendler E, et al. Kaposi’s sarcoma-associated herpesvirus-like DNA sequences in multicentric Castleman’s disease. Blood. 1995;86(4):1276–1280. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
