

Secular trends in colon and rectal cancer relative survival
- PMID: 24174654
- PMCID: PMC3848985
- DOI: 10.1093/jnci/djt299
Secular trends in colon and rectal cancer relative survival
Abstract
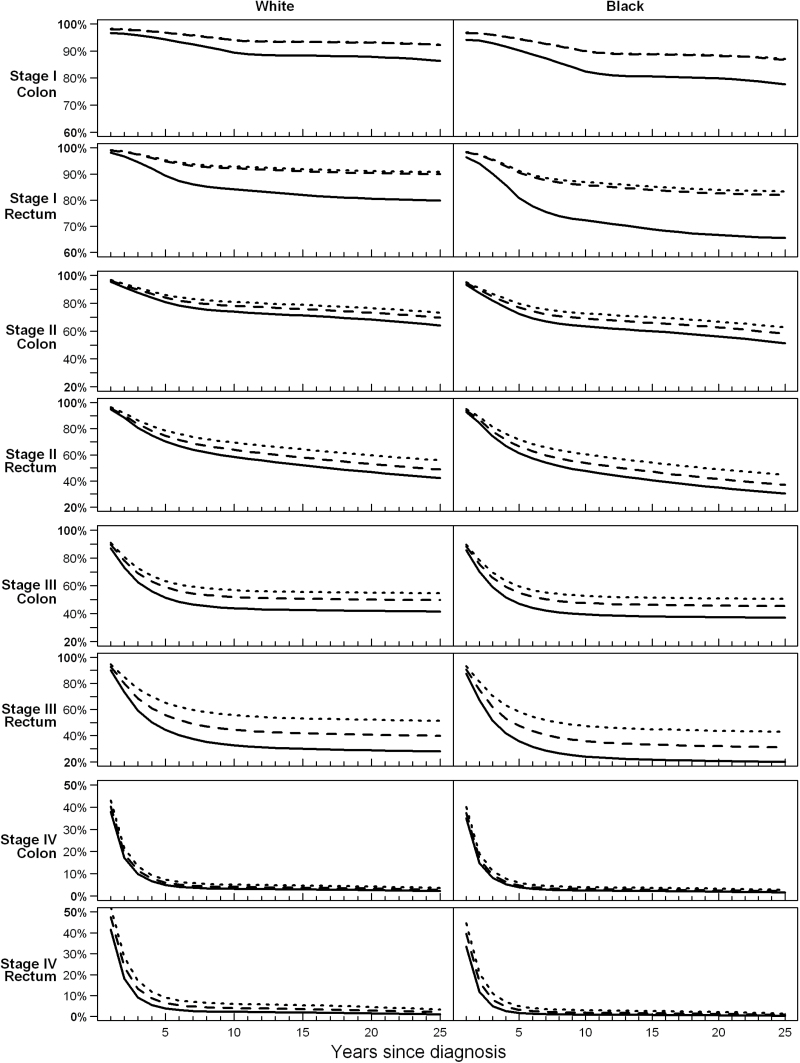
Background: Treatment options for colorectal cancer (CRC) have improved substantially over the past 25 years. Measuring the impact of these improvements on survival outcomes is challenging, however, against the background of overall survival gains from advancements in the prevention, screening, and treatment of other conditions. Relative survival is a metric that accounts for these concurrent changes, allowing assessment of changes in CRC survival. We describe stage- and location-specific trends in relative survival after CRC diagnosis.
Methods: We analyzed survival outcomes for 233965 people in the Surveillance Epidemiology and End Results (SEER) program who were diagnosed with CRC between January 1, 1975, and December 31, 2003. All models were adjusted for sex, race (black vs white), age at diagnosis, time since diagnosis, and diagnosis year. We estimated the proportional difference in survival for CRC patients compared with overall survival for age-, sex-, race-, and period-matched controls to account for concurrent changes in overall survival using two-sided Wald tests.
Results: We found statistically significant reductions in excess hazard of mortality from CRC in 2003 relative to 1975, with excess hazard ratios ranging from 0.75 (stage IV colon cancer; P < .001) to 0.32 (stage I rectal cancer; P < .001), indicating improvements in relative survival for all stages and cancer locations. These improvements occurred in earlier years for patients diagnosed with stage I cancers, with smaller but continuing improvements for later-stage cancers.
Conclusions: Our results demonstrate a steady trend toward improved relative survival for CRC, indicating that treatment and surveillance improvements have had an impact at the population level.
Figures
References
-
- de Gramont A, Chibaudel B, Larsen AK, Tournigand C, Andre T, Gercor French Oncology Research Group. The evolution of adjuvant therapy in the treatment of early-stage colon cancer. Clin Colorectal Cancer. 2011;10(4):218–226. - PubMed
-
- Graham JS, Cassidy J. Adjuvant therapy in colon cancer. Expert Rev Anticancer Ther. 2012;12(1):99–109. - PubMed
-
- Adjuvant Therapy for Patients with Colon and Rectum Cancer. NIH Consensus Development Conference Statement, April 16–18, 1990. http://consensus.nih.gov/1990/1990adjuvanttherapycolonrectalcancer079htm... Accessed September 27, 2013. - PubMed
-
- Saltz LB, Cox JV, Blanke C, et al. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. Irinotecan Study Group. N Engl J Med. 28 2000;343(13):905–914. - PubMed
-
- Goldberg RM, Sargent DJ, Morton RF, et al. A randomized controlled trial of fluorouracil plus leucovorin, irinotecan, and oxaliplatin combinations in patients with previously untreated metastatic colorectal cancer. J Clin Oncol. 2004;22(1):23–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
