

Case Reports
doi: 10.1258/cvd.2012.012006.
eCollection 2012.
Diagnostic confusion resolved by being upbeat
Affiliations
- PMID: 24175063
- PMCID: PMC3738323
- DOI: 10.1258/cvd.2012.012006
Item in Clipboard
Case Reports
Diagnostic confusion resolved by being upbeat
JRSM Cardiovasc Dis.
.
Abstract
The classical stroke presentation - captured by the public health campaign mnemonic FAST (face, arm, speech, time) - does not apply in a large number of stroke cases; yet establishing a prompt diagnosis is imperative for optimal management. Here, we describe a patient with acute bulbar weakness, numbness in all extremities and an apparently normal magnetic resonance imaging (MRI) of the brain upon admission for whom even the fundamental question of whether this reflected a central or peripheral nervous system process was unclear. The critical localizing sign was upbeat nystagmus that denotes a brainstem cause. MRI of the brain in the second week confirmed a diagnosis of medial medullary infarction.
Figures
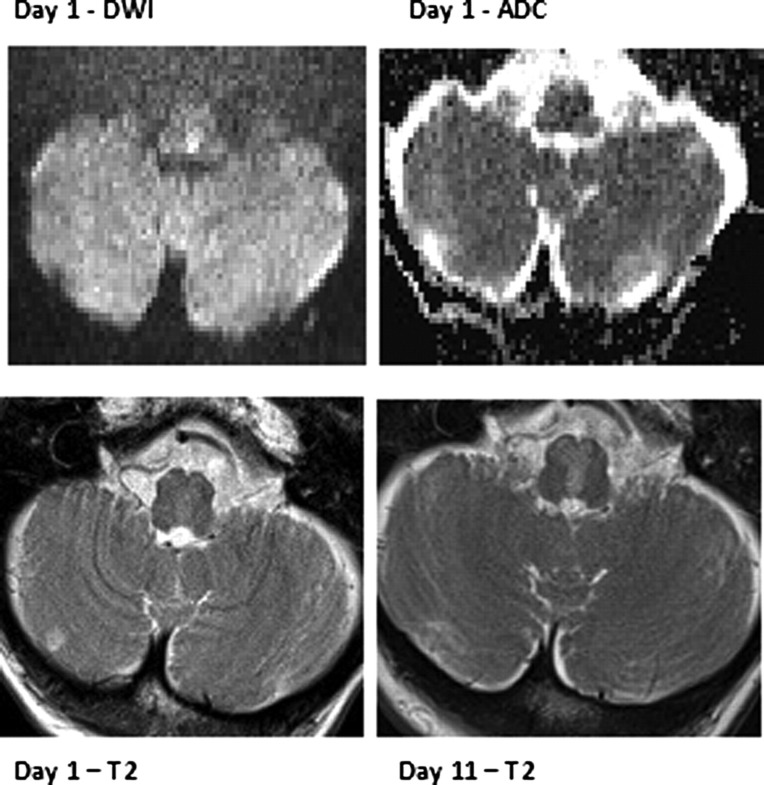
Representative MRI from the patient on admission shows a single voxel of hyperintensity on DWI in dorsal paramedian medulla, equivocal hypointensity of the equivalent apparent diffusion co-efficient (ADC) voxel and subtle hyperintensity of the medial medulla at the same time point. In the second week, a repeat MRI shows unequivocal T2 hyperintensity within a paramedian medullary distribution
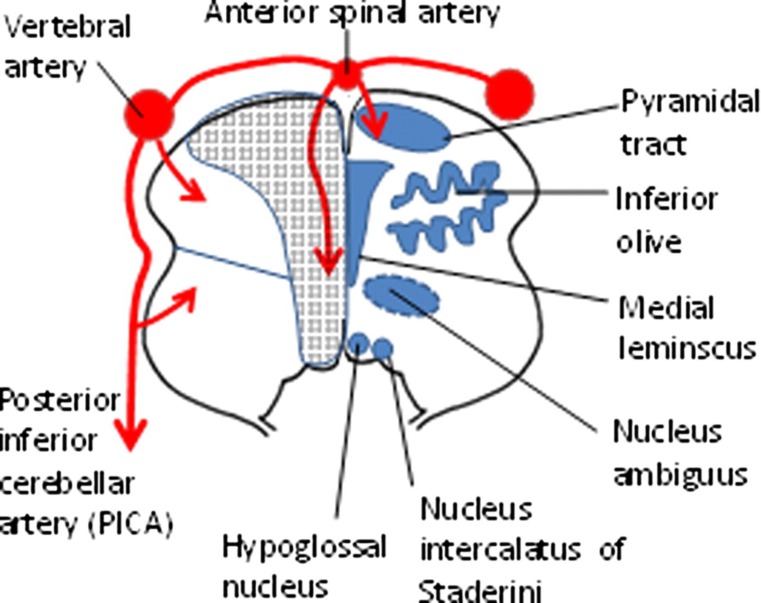
Schematic neuroanatomy of the medulla showing, on the left side, the arterial supply and arterial territories (note similarity of medial medullary artery territory with patient's T2 lesion). On the right side, the most relevant anatomical structures for this case are shown, including nucleus intercalatus which acts as a neural integrator for vertical eye movements; medial lemniscus which conveys spinothalamic fibres; and nucleus ambiguus which conveys efferent vagal fibres to swallowing muscles
Similar articles
-
[Medial medullary infarction: report of three patients presented with central vestibular dysfunction without limb and lingual weakness].Rinsho Shinkeigaku. 1999 Oct;39(10):1059-63. Rinsho Shinkeigaku. 1999. PMID: 10655770 Review. Japanese.
-
Upbeat nystagmus: clinicoanatomical correlations in 15 patients.J Clin Neurol. 2006 Mar;2(1):58-65. doi: 10.3988/jcn.2006.2.1.58. Epub 2006 Mar 20. J Clin Neurol. 2006. PMID: 20396486 Free PMC article.
-
BE-FAST (Balance, Eyes, Face, Arm, Speech, Time): Reducing the Proportion of Strokes Missed Using the FAST Mnemonic.Stroke. 2017 Feb;48(2):479-481. doi: 10.1161/STROKEAHA.116.015169. Epub 2017 Jan 12. Stroke. 2017. PMID: 28082668
-
Primary Position Upbeat Nystagmus during an Acute Attack of Multiple Sclerosis.J Clin Neurol. 2014 Jan;10(1):37-41. doi: 10.3988/jcn.2014.10.1.37. Epub 2014 Jan 6. J Clin Neurol. 2014. PMID: 24465261 Free PMC article.
-
Central oculomotor disturbances and nystagmus: a window into the brainstem and cerebellum.Dtsch Arztebl Int. 2011 Mar;108(12):197-204. doi: 10.3238/arztebl.2011.0197. Epub 2011 Mar 25. Dtsch Arztebl Int. 2011. PMID: 21505601 Free PMC article. Review.
References
-
- Mori M, Kuwabara S, Fukutake T, Yuki N, Hattori T Clinical features and prognosis of Miller Fisher syndrome. Neurology 2001;56:1104–6 - PubMed
-
- Derakhshan I, Lotfi J, Kaufman B Ophthalmoplegia, ataxia and hyporeflexia (Fisher's syndrome). With a midbrain lesion demonstrated by CT scanning. Eur Neurol 1979;18:361–6 - PubMed
-
- Ito K, Mizutani J, Murofushi T, Mizuno M Bilateral pseudointernuclear ophthalmoplegia in myasthenia gravis. ORL J Otorhinolaryngol Relat Spec 1997;59:122–6 - PubMed
-
- Lee SH, Kim DE, Song EC, Roh JK Sensory dermatomal representation in the medial lemniscus. Arch Neurol 2001;58:649–51 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
