

Pitching mechanics, revisited
Abstract
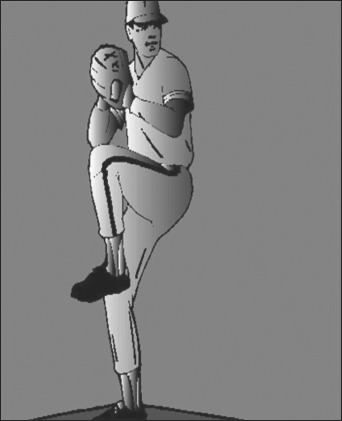
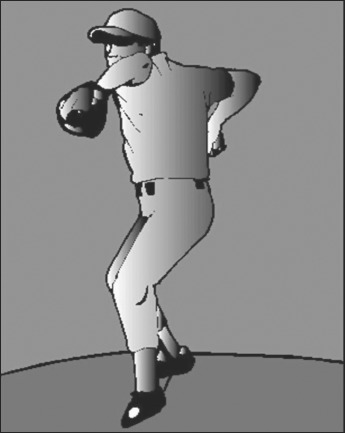
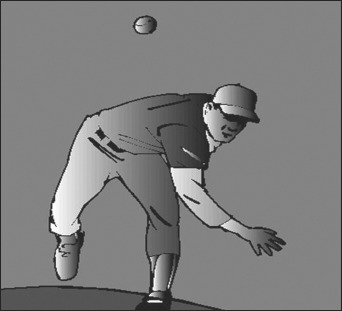
The overhead pitching motion is described as a coordinated sequence of body movements and muscular forces that have an ultimate goal of achieving high ball velocity and target accuracy. An understanding of the dynamic overhead throwing motion outlined in this clinical commentary can assist the clinician in addressing the unique injuries experienced by the pitcher. The potential biomechanical sources for injury have been studied utilizing videography and electromyographic techniques due to the rapid pace with which the pitching motion occurs. This clinical comentary will describe what is widely accepted as the six phases of the pitching motion and the relationship to the kinetic chain theory as well as outline the common mechanical faults that can lead to increased tissue stress and potential injury.
Level of evidence: 5.
Keywords: baseball; overhead athlete; pitching mechanics.
Figures



Similar articles
-
Shoulder Injuries in the Overhead Throwing Athlete.Hand Clin. 2017 Feb;33(1):19-34. doi: 10.1016/j.hcl.2016.08.014. Hand Clin. 2017. PMID: 27886835 Review.
-
The kinetic chain in overhand pitching: its potential role for performance enhancement and injury prevention.Sports Health. 2010 Mar;2(2):135-46. doi: 10.1177/1941738110362656. Sports Health. 2010. PMID: 23015931 Free PMC article.
-
Pitching biomechanics as a pitcher approaches muscular fatigue during a simulated baseball game.Am J Sports Med. 2007 Jan;35(1):23-33. doi: 10.1177/0363546506293025. Epub 2006 Sep 14. Am J Sports Med. 2007. PMID: 16973902
-
Biomechanical comparison of the interval throwing program and baseball pitching: upper extremity loads in training and rehabilitation.Am J Sports Med. 2014 May;42(5):1226-32. doi: 10.1177/0363546514526152. Epub 2014 Mar 24. Am J Sports Med. 2014. PMID: 24664135
-
The Kinetic Chain Revisited: New Concepts on Throwing Mechanics and Injury.PM R. 2016 Mar;8(3 Suppl):S69-77. doi: 10.1016/j.pmrj.2015.11.015. PM R. 2016. PMID: 26972269 Review.
Cited by
-
The Reliability and Validity of a Novel Clinical Test for Assessing Shoulder Rotation ROM in Collegiate Baseball Players: Functional Assessment of System Tension of the Shoulder (FAST-SHDR).Int J Sports Phys Ther. 2024 Dec 1;19(12):1532-1540. doi: 10.26603/001c.126062. eCollection 2024. Int J Sports Phys Ther. 2024. PMID: 39628776 Free PMC article.
-
The Association of Baseball Pitch Delivery and Kinematic Sequence on Stresses at the Shoulder and Elbow Joints.J Sports Sci Med. 2021 Mar 1;20(1):94-100. doi: 10.52082/jssm.2021.94. eCollection 2021 Mar. J Sports Sci Med. 2021. PMID: 33707992 Free PMC article.
-
Throwing Injury Prevention Strategies with a Whole Kinetic Chain-Focused Approach.Curr Rev Musculoskelet Med. 2022 Apr;15(2):53-64. doi: 10.1007/s12178-022-09744-9. Epub 2022 Apr 7. Curr Rev Musculoskelet Med. 2022. PMID: 35389192 Free PMC article. Review.
-
A Clinician's Guide to Analysis of the Pitching Motion.Curr Rev Musculoskelet Med. 2019 Jun;12(2):98-104. doi: 10.1007/s12178-019-09556-4. Curr Rev Musculoskelet Med. 2019. PMID: 31062292 Free PMC article. Review.
-
The Relationship Between Hip Range of Motion and Pitching Kinematics Related to Increased Elbow Valgus Loads in Collegiate Baseball Pitchers: A Pilot Study.Int J Sports Phys Ther. 2021 Apr 1;16(2):468-476. doi: 10.26603/001c.21319. Int J Sports Phys Ther. 2021. PMID: 33842042 Free PMC article.
References
-
- Chen FS, Diaz VA, Loebenberg M, Rosen JE. Shoulder and elbow injuries in the skeletally immature athlete. J Am Acad Orthop Surg. 2005;13:172–185 - PubMed
-
- Grana WA, Rashkin A. Pitcher’s elbow in adolescents. Am J Sports Med. 1980;8:333–336 - PubMed
-
- Limpisvasti O, ElAttrache NS, Jobe FW. Understanding shoulder and elbow injuries in baseball. J Am Acad Orthop Surg. 2007;15:139–147 - PubMed
-
- Olsen SJ II, Fleisig GS, Dun S, Loftice J, Andrews JR. Risk factors for shoulder and elbow injuries in adolescent baseball pitchers. Am J Sports Med. 2006;34:905–912 - PubMed
-
- Fleisig G, Andrews J, Dillman C, Escamilla R. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23:233–239 - PubMed
LinkOut - more resources
Full Text Sources
Research Materials