

Adherence to guideline recommendations for antiarrhythmic drugs in atrial fibrillation
- PMID: 24176443
- PMCID: PMC3818098
- DOI: 10.1016/j.ahj.2013.08.010
Adherence to guideline recommendations for antiarrhythmic drugs in atrial fibrillation
Abstract
Background: Atrial fibrillation (AF) guideline recommendations for antiarrhythmic drugs (AADs) are based on the effectiveness and safety of the AAD in patients with selected, concomitant heart disease. It is unknown to what extent these recommendations are being implemented in clinical practice.
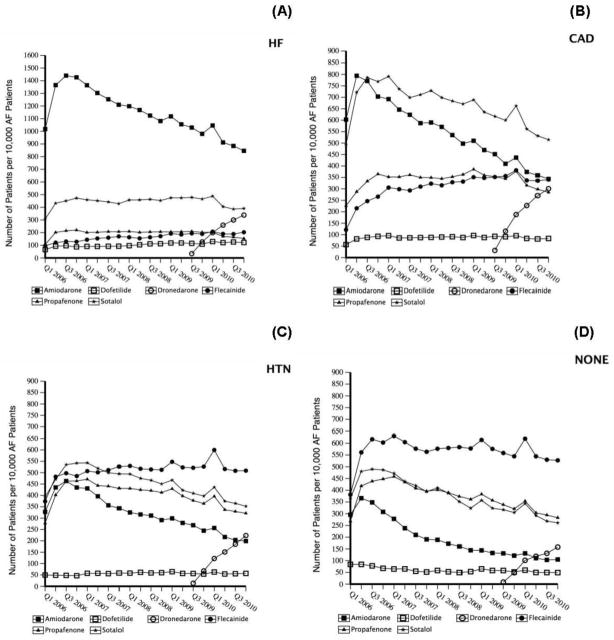
Methods: Using commercial health claims, patients with AF were identified and then categorized into mutually exclusive, guideline-established subgroups based on their most serious concurrent heart disease: heart failure, coronary artery disease (CAD), hypertension, and no heart disease. Antiarrhythmic drug use after the first AF encounter and the identified concurrent heart disease encounter was determined from prescription claims, and this was compared with guideline recommendations.
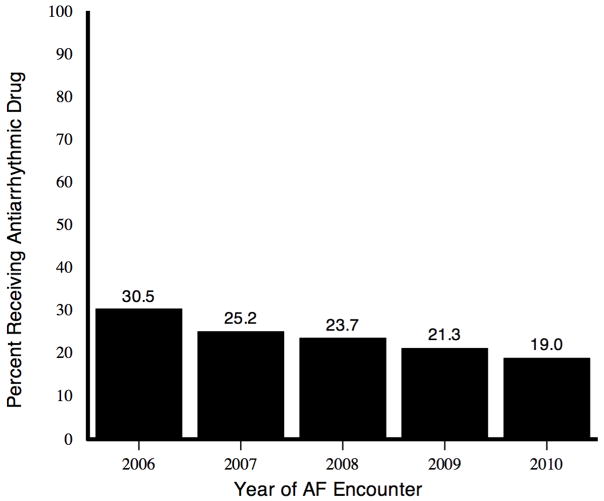
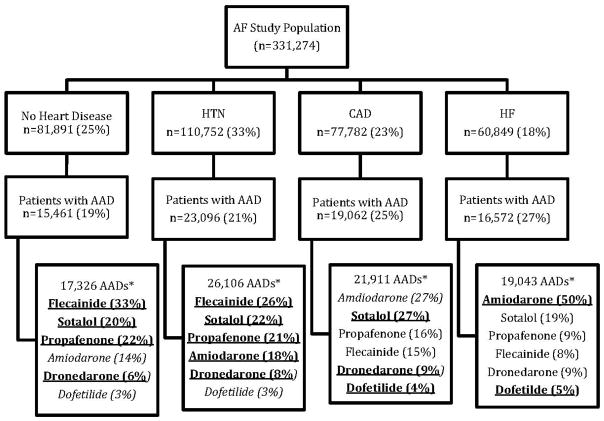
Results: From January 2006 through December 2010, a total of 331,274 patients with AF aged < 65 years were identified: 18%, heart failure; 23%, CAD; 33%, hypertension; and 25%, no heart disease. Of these, 78,877 (24%) patients filled ≥ 1 qualifying AAD prescription. The median age was 57 years (interquartile range 52-61), and 69% were male. A total of 74,191 patients had AADs after both the AF and concurrent heart disease encounters: 27% with heart failure, 25% with CAD, 21% with hypertension, and 19% with no heart disease. In the heart failure and CAD subgroups, 45% and 31% of AADs were inconsistent with first- or second-line guideline recommendations, respectively.
Conclusion: More than one-third of the AADs used in patients with AF and CAD or heart failure did not conform to guideline recommendations. This highlights the potential need for increased clinician education and intervention to improve the safe use of AADs for AF management.
© 2013.
Figures
References
-
- Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114(2):119–25. - PubMed
-
- Go AS, Mozaffarian D, Roger VL, et al. Executive summary: heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013;127(1):143–52. - PubMed
-
- Fuster V, Ryden LE, Cannom DS, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2011;123(10):e269–367. - PubMed
-
- Wann LS, Curtis AB, January CT, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (Updating the 2006 Guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2011;57(2):223–42. - PubMed
-
- Naccarelli GV, Johnston SS, Dalal M, et al. Rates and implications for hospitalization of patients ≥65 years of age with atrial fibrillation/flutter. Am J Cardiol. 2012;109(4):543–9. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
