

Prevention and treatment of postmenopausal osteoporosis
- PMID: 24176761
- PMCID: PMC4187361
- DOI: 10.1016/j.jsbmb.2013.09.008
Prevention and treatment of postmenopausal osteoporosis
Abstract
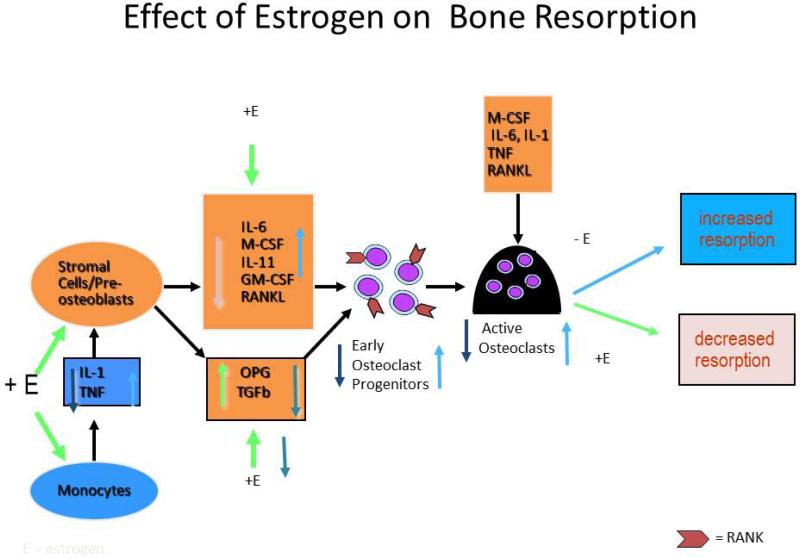
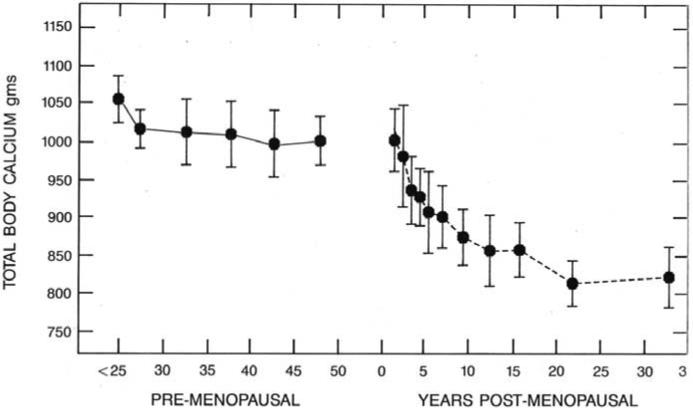
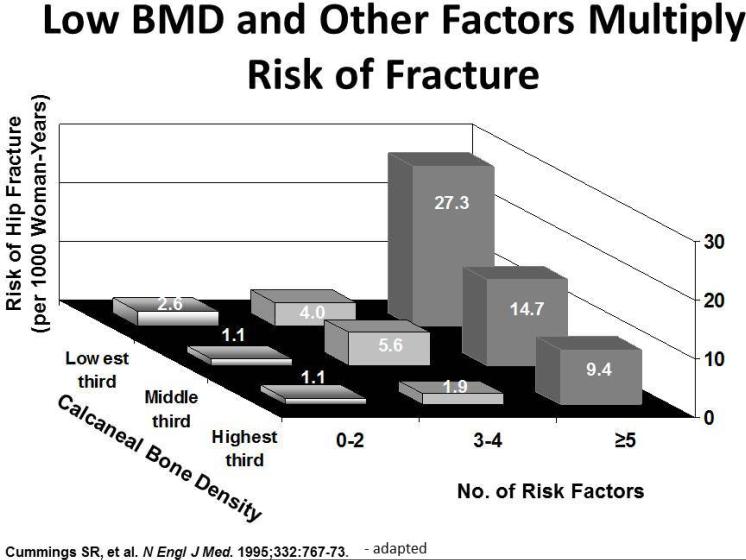
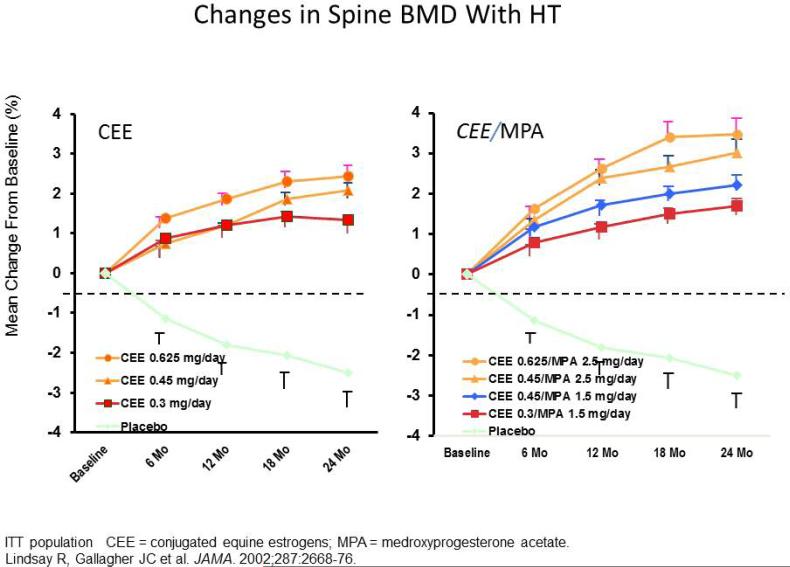
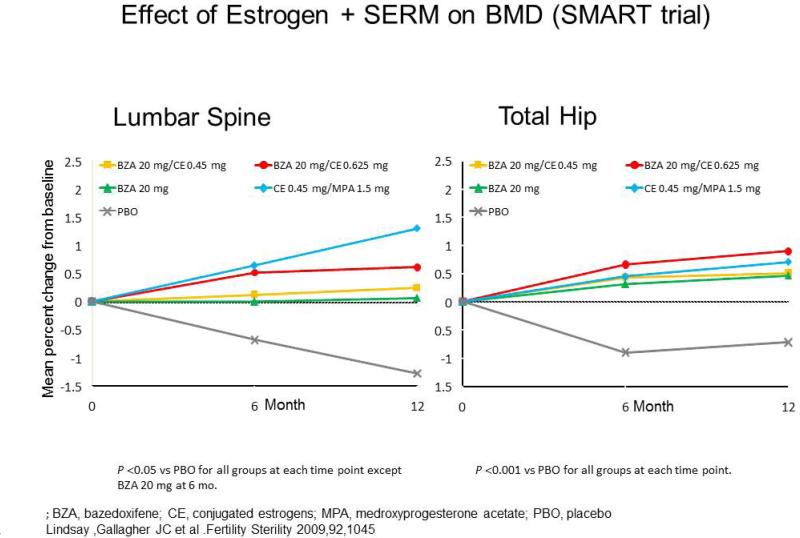
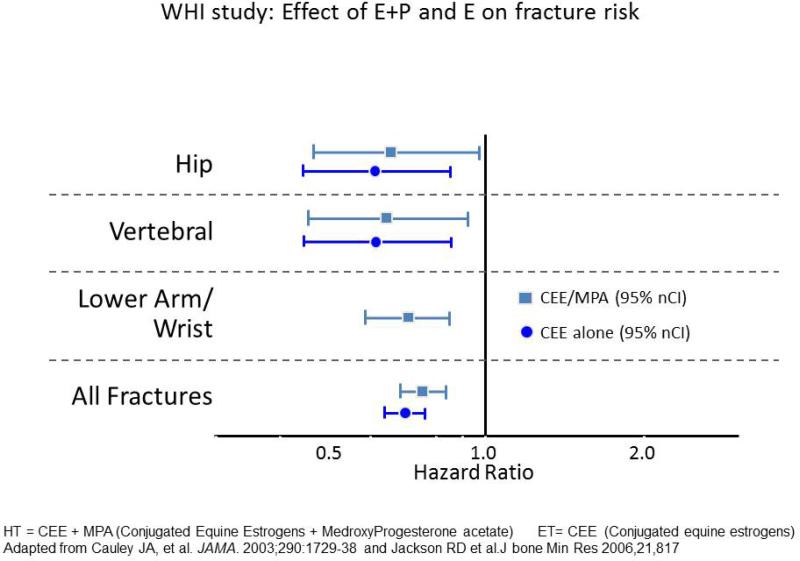
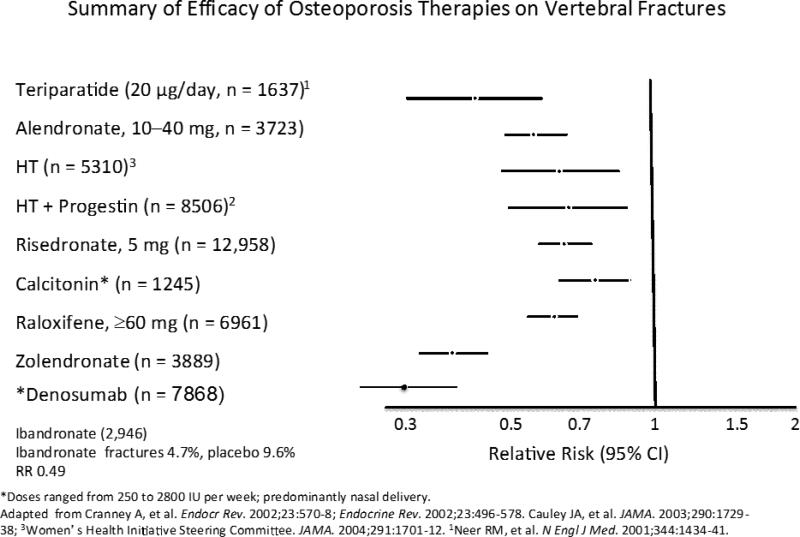
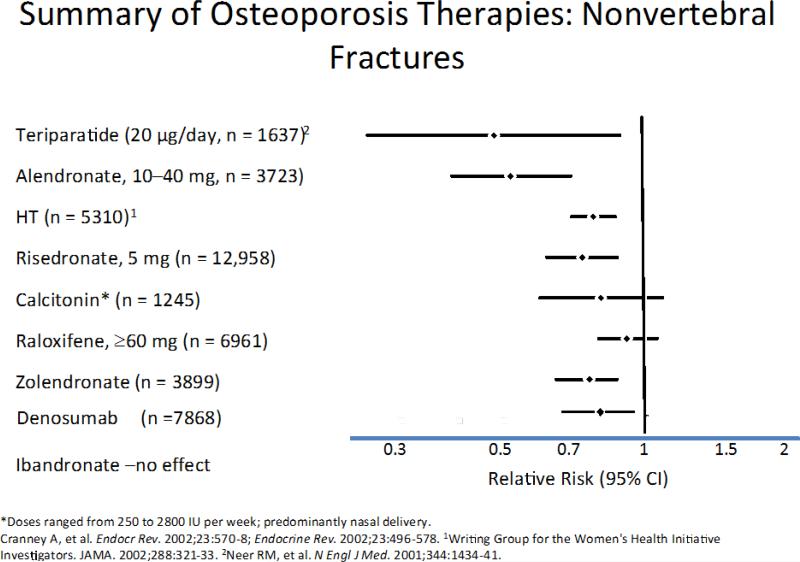
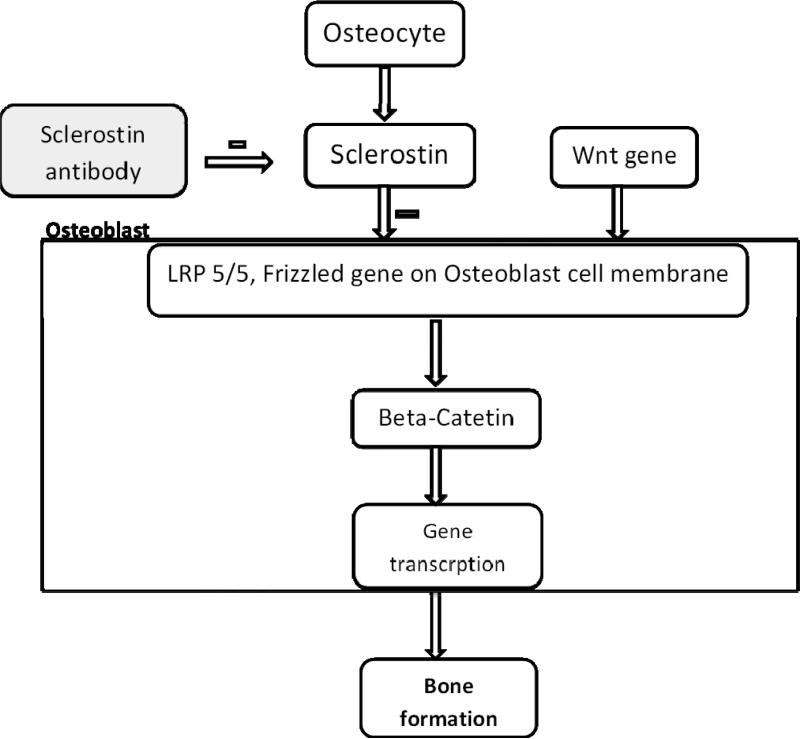
In the beginning, that is from the 1960's, when a link between menopause and osteoporosis was first identified; estrogen treatment was the standard for preventing bone loss, however there was no fracture data, even though it was thought to be effective. This continued until the Women's Health Initiative (WHI) study in 2001 that published data on 6 years of treatment with hormone therapy that showed an increase in heart attacks and breast cancer. Even though the risks were small, 1 per 1500 users annually, patients were worried and there was a large drop off in estrogen use. In later analyses the WHI study showed that estrogen reduced fractures and actually prevented heart attacks in the 50-60 year age group. Estrogen alone appeared to be safer to use than estrogen+the progestin medroxyprogesterone acetate and actually reduced breast cancer. At the same time other drugs were being developed for bone that belong to the bisphosphonate group and the first generation of compounds showed moderate potency on bone resorption. The second and third generation compounds were much more potent and in a series of large trials were shown to reduce fractures. For the last 15 years the treatment of osteoporosis belonged to the bisphosphonate compounds, most of which reduce fracture rates by 50 percent. With the exception of gastrointestinal irritation the drugs are well tolerated and highly effective. The sophistication of the delivery systems now allow treatment that can be given daily, weekly, monthly and annually either orally or intravenously. Bone remodeling is a dynamic process that repairs microfractures and replaces old bone with new bone. In the last 10 years there has been a remarkable understanding of bone biology so that new therapies can be specifically designed on a biological basis. The realization that RANKL was the final cytokine involved in the resorption process and that marrow cells produced a natural antagonist called Osteoprotegerin (OPG) quickly led to two lines of therapy. First OPG was used as a therapy to block RANKL was initially successful but later antibodies against OPG developed and this line of treatment had to be discontinued. The next step was to develop a monoclonal antibody against RANKL and this proved to be highly effective in blocking bone resorption. It led to development of a drug Denosumab that successfully reduces fractures and is now one of the therapeutic options for osteoporosis treatment. On the anabolic side bone biology research showed that osteocytes produces sclerostin an inhibitor of the anabolic WNT signaling pathway. Recent development of a monoclonal antibody against sclerostin has shown remarkable anabolic activity in bone showing large increases in bone density and fracture trials are now underway. The newer treatments for osteoporosis are likely to be based on our understanding of bone biology and the design of new highly specific compounds with fewer side effects. This review summarizes the diagnosis of postmenopausal osteoporosis and various available non-pharmacological and pharmacological therapies available for its management. This article is part of a Special Issue entitled 'Menopause'.
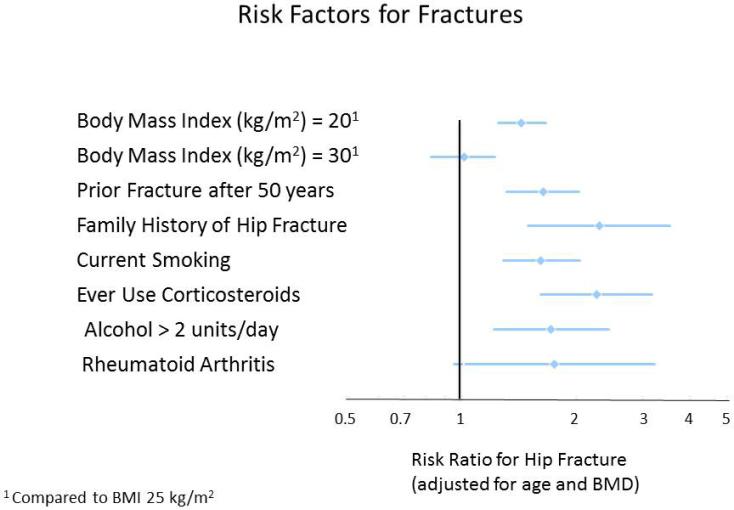
Keywords: BMD; Diagnosis; Osteoporosis; Risk factors; Treatment.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
References
-
- Pacifici R. Estrogen, cytokines, and pathogenesis of postmenopausal osteoporosis. J Bone Miner Res. 1996;11:1043–1051. - PubMed
-
- Riggs BL, Khosla S, Melton LJ., III A unitary model for involutional osteoporosis: estrogen deficiency causes both type I and type II osteoporosis in postmenopausal women and contributes to bone loss in aging men. J. Bone Miner. Res. 1998;13:763–773. - PubMed
-
- Hofbauer LC, et al. The roles of osteoprotegerin and osteoprotegerin ligand in the paracrine regulation of bone resorption. J. Bone Miner. Res. 2000;15:2–12. - PubMed
-
- Bullamore JR, Wilkinson R, Gallagher JC, Nordin BE. Marshall DHEffect of age on calcium absorption. Lancet. 1970 Sep 12;2(7672):535–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
