

Development and validation of a prediction rule using the Oxford classification in IgA nephropathy
- PMID: 24178970
- PMCID: PMC3848397
- DOI: 10.2215/CJN.03480413
Development and validation of a prediction rule using the Oxford classification in IgA nephropathy
Abstract
Background and objectives: The risk assessment for developing ESRD remains limited in patients with IgA nephropathy (IgAN). The aim of this study was to develop and validate a prediction rule for estimating the individual risk of ESRD in patients with IgAN.
Design, setting, participants, & measurements: A total of 698 patients with IgAN diagnosed by renal biopsy at Kyushu University Hospital (derivation cohort) between 1982 and 2010 were retrospectively followed. The Oxford classification was used to evaluate the pathologic lesions. The risk factors for developing ESRD were evaluated using a Cox proportional hazard model with a stepwise backward elimination method. The prediction rule was verified using data from 702 patients diagnosed at Japanese Red Cross Fukuoka Hospital (validation cohort) between 1979 and 2002.
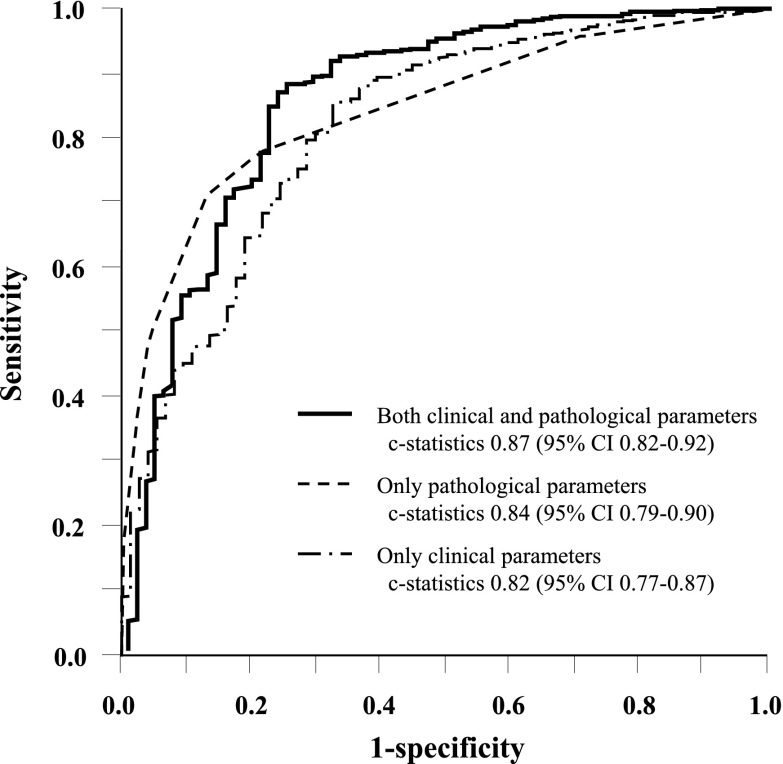
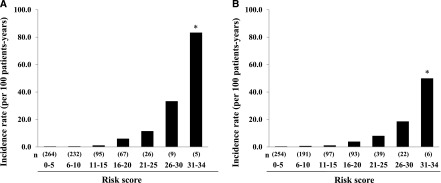
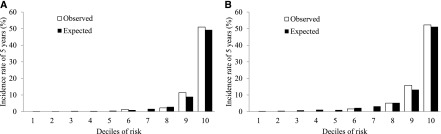
Results: In the derivation cohort, 73 patients developed ESRD during the median 4.7-year follow-up. The final prediction model included proteinuria (hazard ratio [HR], 1.30; 95% confidence interval [95% CI], 1.16 to 1.45, every 1 g/24 hours), estimated GFR (HR, 0.84; 95% CI, 0.74 to 0.96, every 10 ml/min per 1.73 m(2)), mesangial proliferation (HR, 1.85; 95% CI, 1.10 to 3.11), segmental sclerosis (HR, 3.21; 95% CI, 1.37 to 7.51), and interstitial fibrosis/tubular atrophy (T1: HR, 5.30; 95% CI, 2.63 to 10.7; T2: HR, 20.5; 95% CI, 9.05 to 46.5) as independent risk factors for developing ESRD. To create a prediction rule, the score for each variable was weighted by the regression coefficients calculated using the relevant Cox model. The incidence of ESRD increased linearly with increases in the total risk scores (P for trend <0.001). Furthermore, the prediction rule demonstrated good discrimination (c-statistic=0.89) and calibration (Hosmer-Lemeshow test, P=0.78) in the validation cohort.
Conclusions: This study developed and validated a new prediction rule using clinical measures and the Oxford classification for developing ESRD in patients with IgAN.
Figures
References
-
- D’Amico G: The commonest glomerulonephritis in the world: IgA nephropathy. Q J Med 64: 709–727, 1987 - PubMed
-
- Lv J, Zhang H, Zhou Y, Li G, Zou W, Wang H: Natural history of immunoglobulin A nephropathy and predictive factors of prognosis: A long-term follow up of 204 cases in China. Nephrology (Carlton) 13: 242–246, 2008 - PubMed
-
- Li PK, Ho KK, Szeto CC, Yu L, Lai FM: Prognostic indicators of IgA nephropathy in the Chinese—clinical and pathological perspectives. Nephrol Dial Transplant 17: 64–69, 2002 - PubMed
-
- Radford MG, Jr, Donadio JV, Jr, Bergstralh EJ, Grande JP: Predicting renal outcome in IgA nephropathy. J Am Soc Nephrol 8: 199–207, 1997 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
