

Incidence, outcomes, and comparisons across definitions of AKI in hospitalized individuals
- PMID: 24178971
- PMCID: PMC3878695
- DOI: 10.2215/CJN.02730313
Incidence, outcomes, and comparisons across definitions of AKI in hospitalized individuals
Abstract
Background and objectives: At least four definitions of AKI have recently been proposed. This study sought to characterize the epidemiology of AKI according to the most recent consensus definition proposed by the Kidney Disease Improving Global Outcomes (KDIGO) Work Group, and to compare it with three other definitions.
Design, setting, participants, & measurements: This was a retrospective cohort study of 31,970 hospitalizations at an academic medical center in 2010. AKI was defined and staged according to KDIGO criteria, the Acute Dialysis Quality Initiative's RIFLE criteria, the Acute Kidney Injury Network (AKIN) criteria, and a definition based on a model of creatinine kinetics (CK). Outcomes of interest were incidence, in-hospital mortality, length of stay, costs, readmission rates, and posthospitalization disposition.
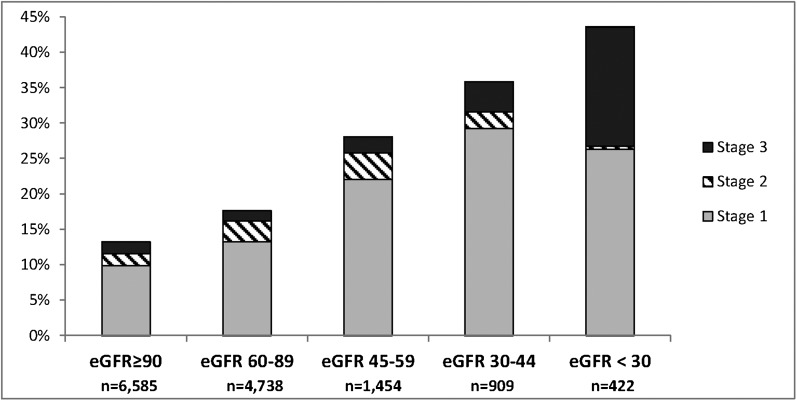
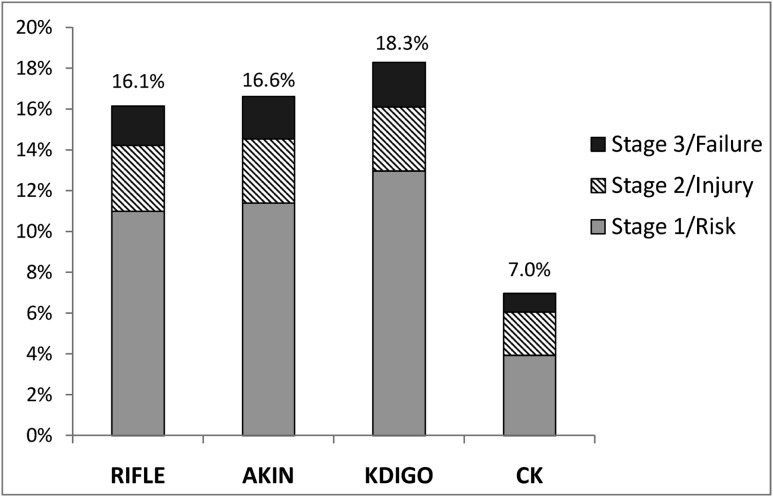
Results: AKI incidence was highest according to the KDIGO definition (18.3%) followed by the AKIN (16.6%), RIFLE (16.1%), and CK (7.0%) definitions. AKI incidence appeared markedly higher in those with low baseline serum creatinine according to the KDIGO, AKIN, and RIFLE definitions, in which AKI may be defined by a 50% increase over baseline. AKI according to all definitions was associated with a significantly higher risk of death and higher resource utilization. The adjusted odds ratios for in-hospital mortality in those with AKI were highest with the CK definition (5.2; 95% confidence interval [95% CI], 4.1 to 6.6), followed by the RIFLE (2.9; 95% CI, 2.2 to 3.6), KDIGO (2.8; 95% CI, 2.2 to 3.6), and AKIN (2.6; 95% CI, 2.0 to 3.3) definitions. Concordance in diagnosis and staging was high among the KDIGO, AKIN, and RIFLE definitions.
Conclusions: The incidence of AKI in hospitalized individuals varies depending on the definition used. AKI according to all definitions is associated with higher in-hospital mortality and resource utilization. AKI may be inappropriately diagnosed in those with low baseline serum creatinine using definitions that incorporate percentage increases over baseline.
Figures
References
-
- Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW: Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol 16: 3365–3370, 2005 - PubMed
-
- Parikh A, Shaw A: The economics of renal failure and kidney disease in critically ill patients. Crit Care Clin 28: 99–111, vii, 2012 - PubMed
-
- Lahoti A, Nates JL, Wakefield CD, Price KJ, Salahudeen AK: Costs and outcomes of acute kidney injury in critically ill patients with cancer. J Support Oncol 9: 149–155, 2011 - PubMed
-
- Uchino S, Bellomo R, Goldsmith D, Bates S, Ronco C: An assessment of the RIFLE criteria for acute renal failure in hospitalized patients. Crit Care Med 34: 1913–1917, 2006 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
