

C3 glomerulopathy: clinicopathologic features and predictors of outcome
- PMID: 24178974
- PMCID: PMC3878702
- DOI: 10.2215/CJN.04700513
C3 glomerulopathy: clinicopathologic features and predictors of outcome
Abstract
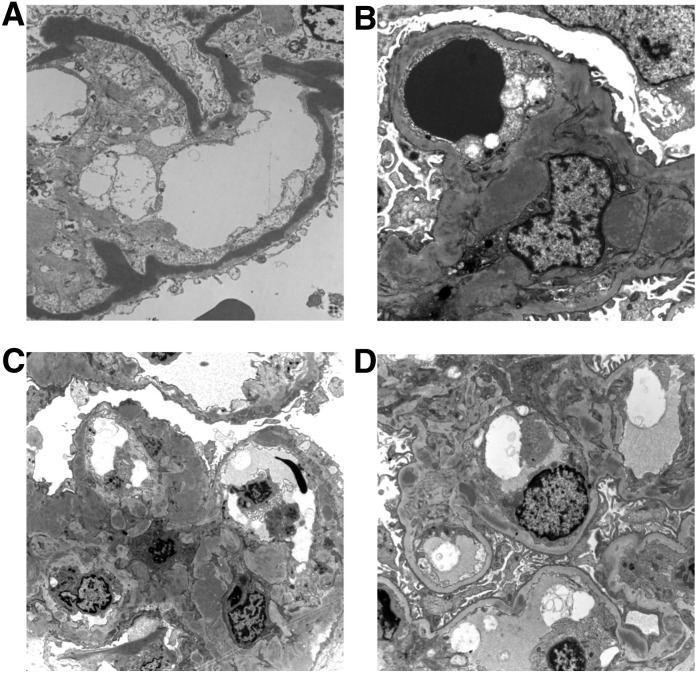
Background and objectives: The term C3 glomerulopathy describes renal disorders characterized by the presence of glomerular deposits composed of C3 in the absence of significant amounts of Ig. On the basis of electron microscopy appearance, subsets of C3 glomerulopathy include dense deposit disease (DDD) and C3 glomerulonephritis (C3GN). The full spectrum of histologic change observed in C3 glomerulopathy has yet to be defined and pathologic predictors of renal outcome within this patient population remain largely unknown. This study thus characterized a large C3 glomerulopathy cohort and identified clinicopathologic predictors of renal outcome.
Design, setting, participants, & measurements: All patients with kidney biopsies fulfilling criteria for C3 glomerulopathy from two quaternary renal centers within the United Kingdom and Ireland between 1992 and 2012 were retrospectively reviewed. We recorded histologic, demographic, and clinical data and determined predictors of ESRD using the Cox proportional hazards model.
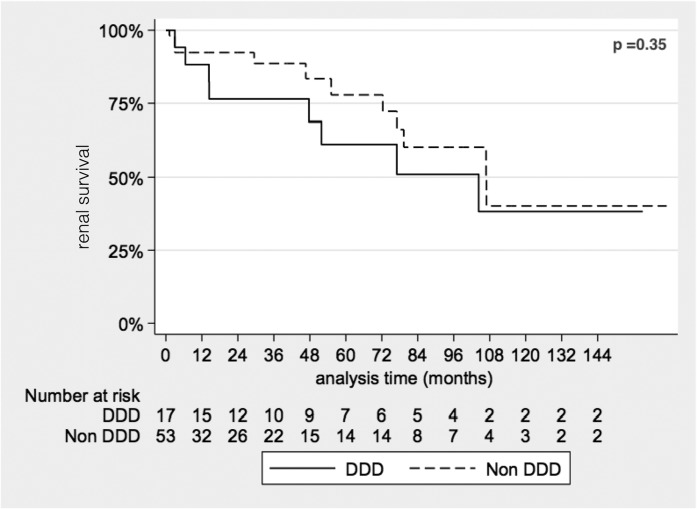
Results: Eighty patients with C3 glomerulopathy were identified: 21 with DDD and 59 with C3GN. Patients with DDD were younger, more likely to have low serum C3 levels, and more likely to have crescentic GN than patients with C3GN. Patients with C3GN were older and had more severe arteriolar sclerosis, glomerular sclerosis, and interstitial scarring than patients with DDD. Of 70 patients with available follow-up data, 20 (29%) progressed to ESRD after a median of 28 months. Age >16 years, DDD subtype, and crescentic GN were independent predictors of ESRD within the entire cohort. Renal impairment at presentation predicted ESRD only among patients with DDD.
Conclusions: Although detailed serologic and genetic data are lacking, this study nevertheless identifies important clinicopathologic distinctions between patients with DDD and C3GN. These include independent predictors of renal outcome. If replicated in other cohorts, these predictors could be used to stratify patients, enabling application of emerging mechanism-based therapies to patients at high risk for poor renal outcome.
Figures
References
-
- Walport MJ: Complement. First of two parts. N Engl J Med 344: 1058–1066, 2001 - PubMed
-
- Rodríguez de Córdoba S, Esparza-Gordillo J, Goicoechea de Jorge E, Lopez-Trascasa M, Sánchez-Corral P: The human complement factor H: Functional roles, genetic variations and disease associations. Mol Immunol 41: 355–367, 2004 - PubMed
-
- Haines JL, Hauser MA, Schmidt S, Scott WK, Olson LM, Gallins P, Spencer KL, Kwan SY, Noureddine M, Gilbert JR, Schnetz-Boutaud N, Agarwal A, Postel EA, Pericak-Vance MA: Complement factor H variant increases the risk of age-related macular degeneration. Science 308: 419–421, 2005 - PubMed
-
- Appel GB, Cook HT, Hageman G, Jennette JC, Kashgarian M, Kirschfink M, Lambris JD, Lanning L, Lutz HU, Meri S, Rose NR, Salant DJ, Sethi S, Smith RJ, Smoyer W, Tully HF, Tully SP, Walker P, Welsh M, Würzner R, Zipfel PF: Membranoproliferative glomerulonephritis type II (dense deposit disease): An update. J Am Soc Nephrol 16: 1392–1403, 2005 - PubMed
-
- Fakhouri F, Frémeaux-Bacchi V, Noël LH, Cook HT, Pickering MC: C3 glomerulopathy: A new classification. Nat Rev Nephrol 6: 494–499, 2010 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
