

Association between GFR estimated by multiple methods at dialysis commencement and patient survival
- PMID: 24178976
- PMCID: PMC3878691
- DOI: 10.2215/CJN.02310213
Association between GFR estimated by multiple methods at dialysis commencement and patient survival
Abstract
Background and objectives: The Initiating Dialysis Early and Late study showed that planned early or late initiation of dialysis, based on the Cockcroft and Gault estimation of GFR, was associated with identical clinical outcomes. This study examined the association of all-cause mortality with estimated GFR at dialysis commencement, which was determined using multiple formulas.
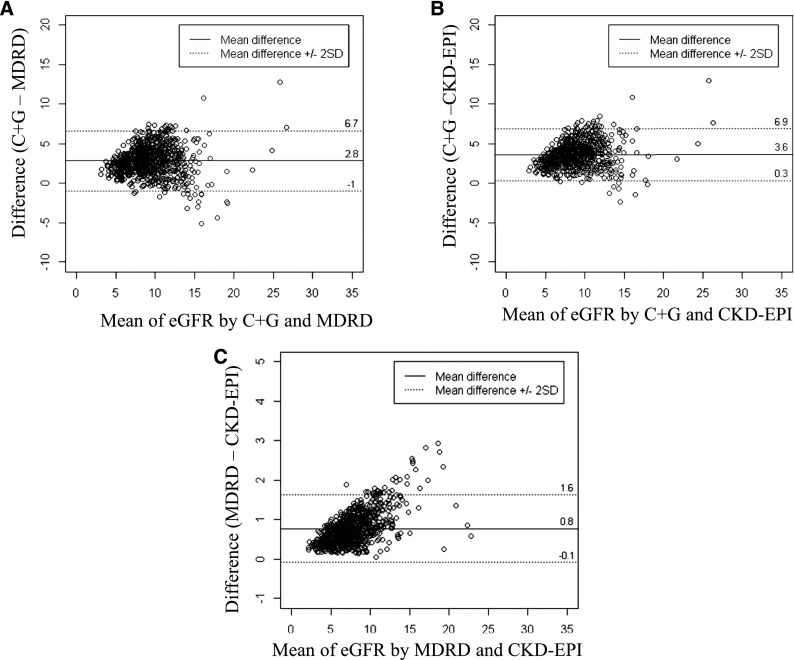
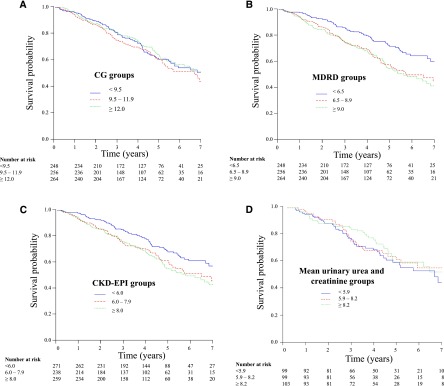
Design, setting, participants, & measurements: Initiating Dialysis Early and Late trial participants were stratified into tertiles according to the estimated GFR measured by Cockcroft and Gault, Modification of Diet in Renal Disease, or Chronic Kidney Disease-Epidemiology Collaboration formula at dialysis commencement. Patient survival was determined using multivariable Cox proportional hazards model regression.
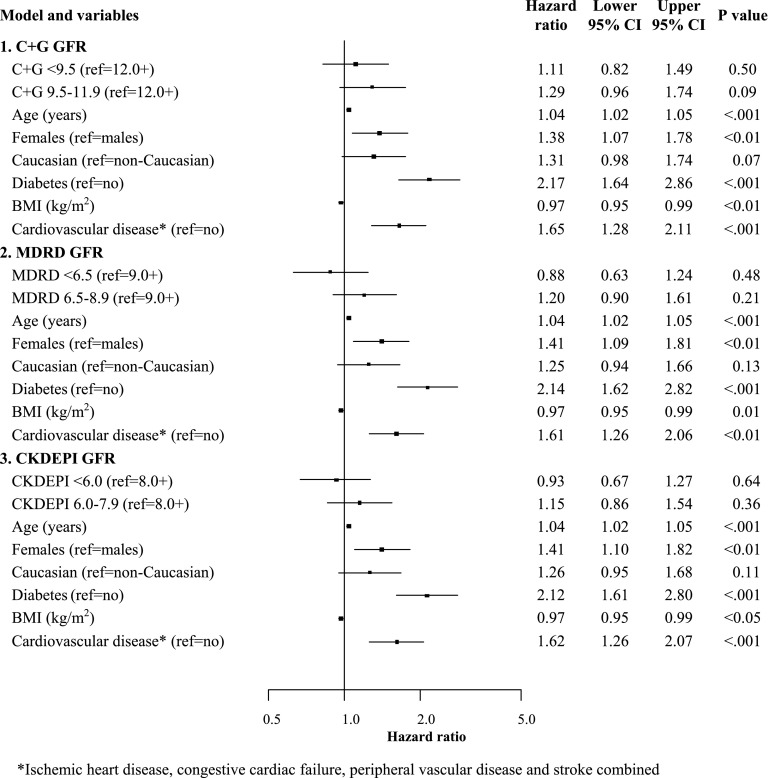
Results: Only Initiating Dialysis Early and Late trial participants who commenced on dialysis were included in this study (n=768). A total of 275 patients died during the study. After adjustment for age, sex, racial origin, body mass index, diabetes, and cardiovascular disease, no significant differences in survival were observed between estimated GFR tertiles determined by Cockcroft and Gault (lowest tertile adjusted hazard ratio, 1.11; 95% confidence interval, 0.82 to 1.49; middle tertile hazard ratio, 1.29; 95% confidence interval, 0.96 to 1.74; highest tertile reference), Modification of Diet in Renal Disease (lowest tertile hazard ratio, 0.88; 95% confidence interval, 0.63 to 1.24; middle tertile hazard ratio, 1.20; 95% confidence interval, 0.90 to 1.61; highest tertile reference), and Chronic Kidney Disease-Epidemiology Collaboration equations (lowest tertile hazard ratio, 0.93; 95% confidence interval, 0.67 to 1.27; middle tertile hazard ratio, 1.15; 95% confidence interval, 0.86 to 1.54; highest tertile reference).
Conclusion: Estimated GFR at dialysis commencement was not significantly associated with patient survival, regardless of the formula used. However, a clinically important association cannot be excluded, because observed confidence intervals were wide.
Figures
References
-
- Bonomini V, Baldrati L, Stefoni S: Comparative cost/benefit analysis in early and late dialysis. Nephron 33: 1–4, 1983 - PubMed
-
- Bonomini V, Albertazzi A, Vangelista A, Bortolotti GC, Stefoni S, Scolari MP: Residual renal function and effective rehabilitation in chronic dialysis. Nephron 16: 89–102, 1976 - PubMed
-
- Bonomini V, Feletti C, Scolari MP, Stefoni S: Benefits of early initiation of dialysis. Kidney Int Suppl 17: S57–S59, 1985 - PubMed
-
- Jungers P, Zingraff J, Albouze G, Chauveau P, Page B, Hannedouche T, Man NK: Late referral to maintenance dialysis: Detrimental consequences. Nephrol Dial Transplant 8: 1089–1093, 1993 - PubMed
-
- Jungers P, Zingraff J, Page B, Albouze G, Hannedouche T, Man NK: Detrimental effects of late referral in patients with chronic renal failure: A case-control study. Kidney Int Suppl 41: S170–S173, 1993 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
