

Solitary infantile myofibromatosis in the bones of the upper extremities: Two rare cases and a review of the literature
- PMID: 24179532
- PMCID: PMC3813798
- DOI: 10.3892/ol.2013.1584
Solitary infantile myofibromatosis in the bones of the upper extremities: Two rare cases and a review of the literature
Abstract
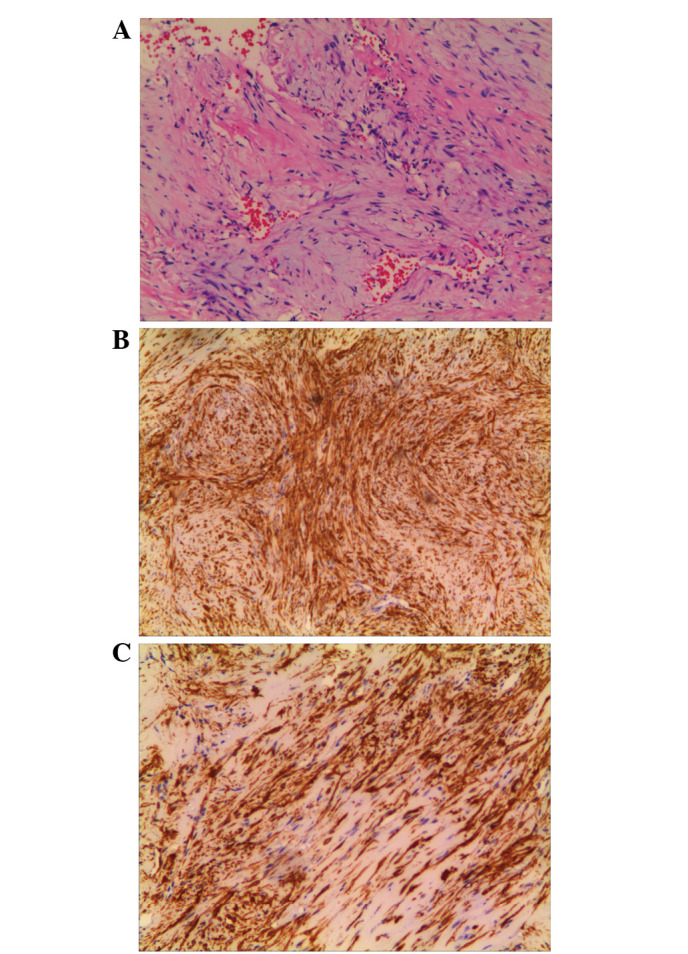
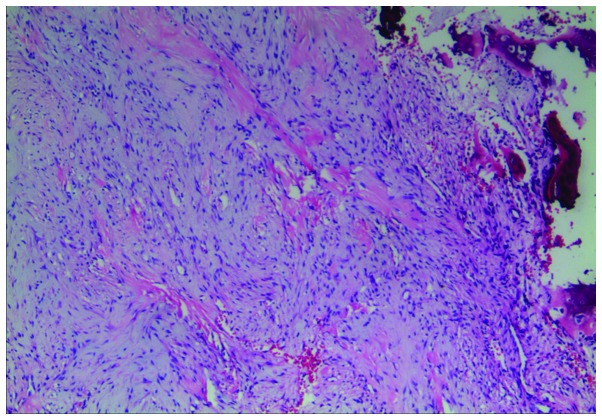
Infantile myofibromatosis (IM) is the most common fibrous tumor of infancy. IM may arise in a solitary or multicentric form, with similar histopathological findings, however, the clinical features and prognoses may vary. The solitary form tends to occur predominantly in males and is typically observed in the dermis, subcutis or deep soft tissues. The reported incidence of solitary osseous myofibromatosis is rare. Furthermore, the majority of solitary IM cases of the bone occur in the craniofacial bones, while the occurrence of solitary osseous myofibromatosis on the extremities has been sporadically reported. The present study describes two cases of solitary IM involving the bones of the upper extremities in females who were over two years old. The cases show unusual symptom presentation and the tumor origin is in a rarely observed location. The study discusses the clinical, radiological and pathological features, in addition to the previously described etiology, prognosis and treatment options for this condition.
Keywords: bone; extremities; humerus; infantile myofibromatosis; solitary; ulna.
Figures

References
-
- Koujok K, Ruiz RE, Hernandez RJ. Myofibromatosis: imaging characteristics. Pediatr Radiol. 2005;35:374–380. - PubMed
-
- Stout AP. Juvenile fibromatoses. Cancer. 1954;7:953–978. - PubMed
-
- Chung EB, Enzinger FM. Infantile myofibromatosis. Cancer. 1981;48:1807–1818. - PubMed
-
- Murphey MD, Ruble CM, Tyszko SM, Zbojniewicz AM, Potter BK, Miettinen M. From the archives of the AFIP: musculoskeletal fibromatoses: radiologic-pathologic correlation. Radiographics. 2009;29:2143–2173. - PubMed
-
- Gatibelza ME, Vazquez BR, Bereni N, Denis D, Bardot J, Degardin N. Isolated infantile myofibromatosis of the upper eyelid: uncommon localization and long-term results after surgical management. J Pediatr Surg. 2012;47:1457–1459. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources