

Ventricular-arterial coupling: Invasive and non-invasive assessment
- PMID: 24179554
- PMCID: PMC3809068
- DOI: 10.1016/j.artres.2012.12.002
Ventricular-arterial coupling: Invasive and non-invasive assessment
Abstract
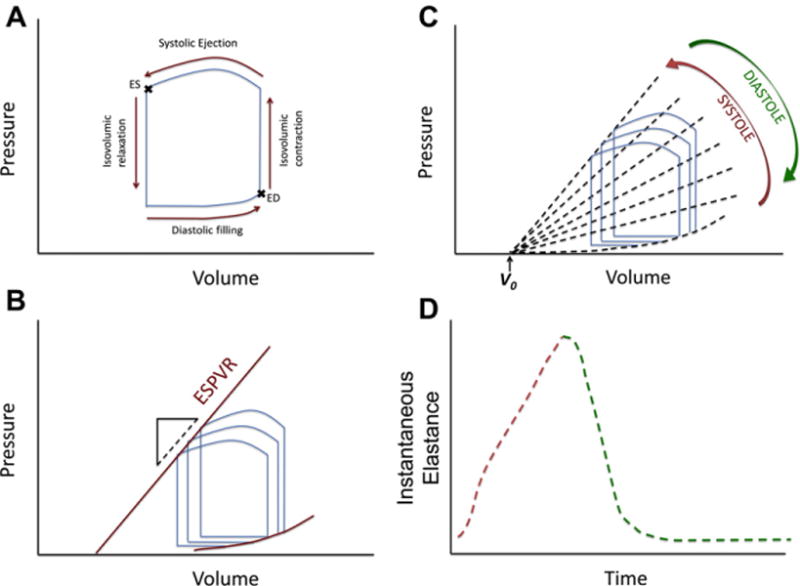
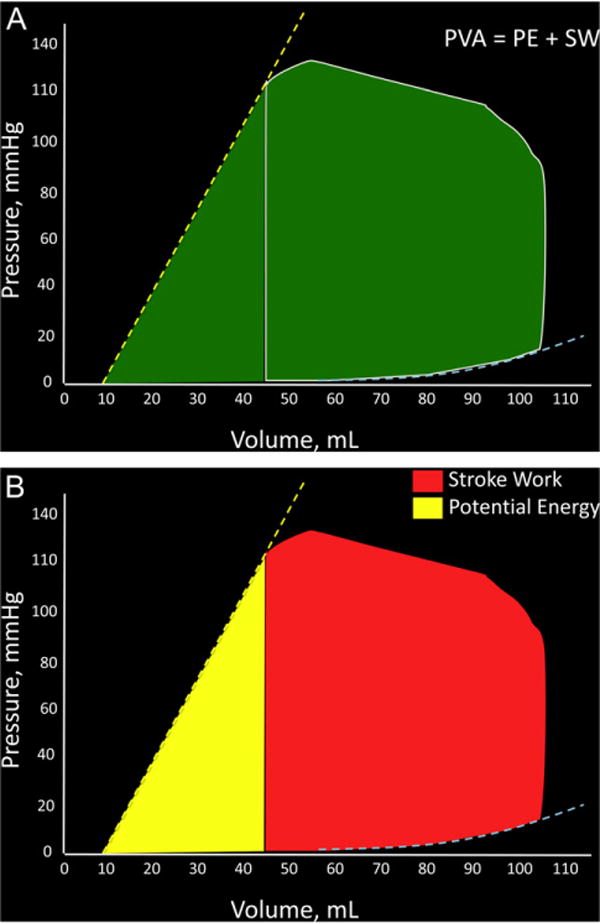
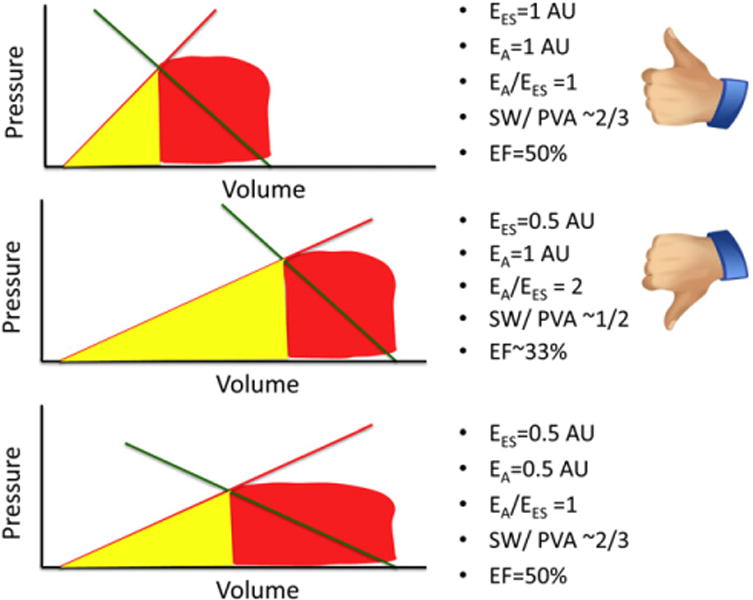
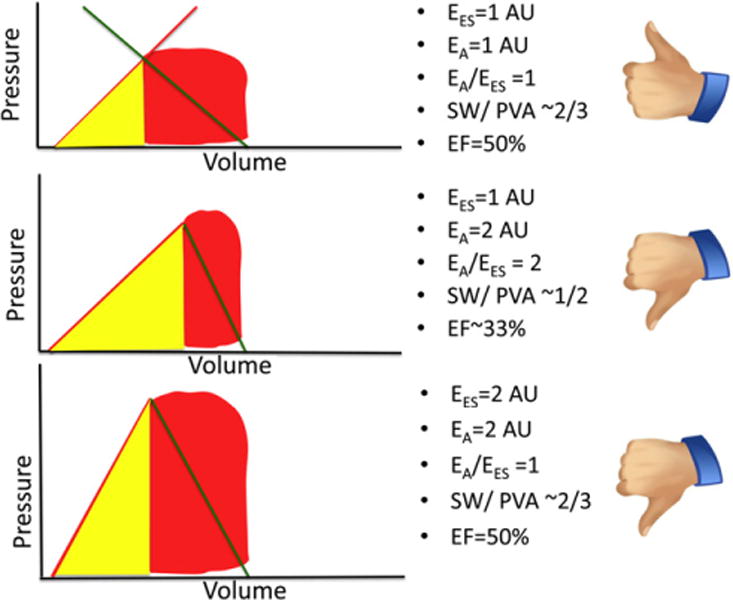
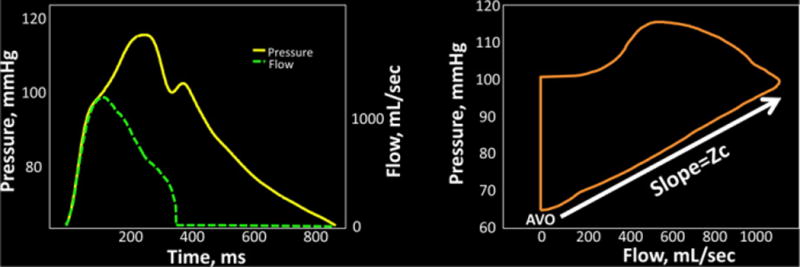
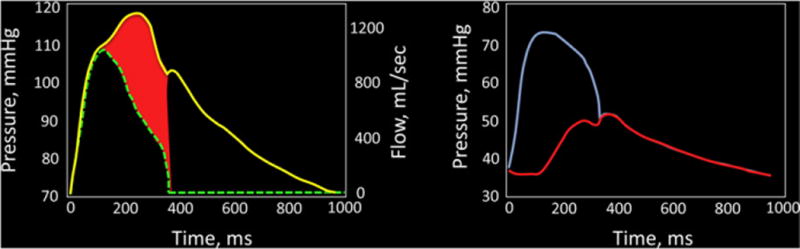
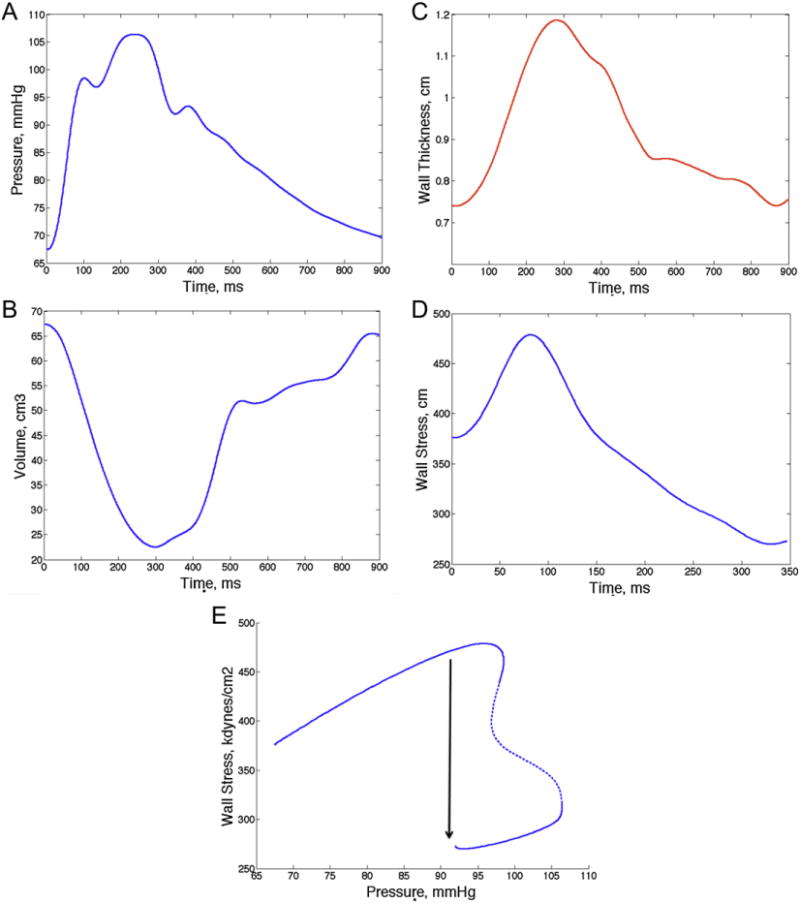
Interactions between the left ventricle (LV) and the arterial system, (ventricular-arterial coupling) are key determinants of cardiovascular function. Ventricularearterial coupling is most frequently assessed in the pressure-volume plane using the ratio of effective arterial elastance (EA) to LV end-systolic elastance (EES). EA (usually interpreted as a lumped index of arterial load) can be computed as end-systolic pressure/stroke volume, whereas EES (a load-independent measure of LV chamber systolic stiffness and contractility) is ideally assessed invasively using data from a family of pressure-volume loops obtained during an acute preload alteration. Single-beat methods have also been proposed, allowing for non-invasive estimations of EES using simple echocardiographic measurements. The EA/EES ratio is useful because it provides information regarding the operating mechanical efficiency and performance of the ventricular-arterial system. However, it should be recognized that analyses in the pressure-volume plane have several limitations and that "ventricular-arterial coupling" encompasses multiple physiologic aspects, many of which are not captured in the pressure-volume plane. Therefore, additional assessments provide important incremental physiologic information about the cardiovascular system and should be more widely used. In particular, it should be recognized that: (1) comprehensive analyses of arterial load are important because EA poorly characterizes pulsatile LV load and does not depend exclusively on arterial properties; (2) The systolic loading sequence, an important aspect of ventricular-arterial coupling, is neglected by pressure-volume analyses, and can profoundly impact LV function, remodeling and progression to heart failure. This brief review summarizes methods for the assessment of ventricular-arterial interactions, as discussed at the Artery 12 meeting (October 2012).
Keywords: Effective arterial elastance; Ventricular afterload; Ventricular elastance; Ventricular-arterial coupling.
Figures
References
-
- Suga H. Theoretical analysis of a left-ventricular pumping model based on the systolic time-varying pressure–volume ratio. IEEE Trans Biomed Eng. 1971;18:47–55. - PubMed
-
- Suga H. Total mechanical energy of a ventricle model and cardiac oxygen consumption. AmJPhysiol. 1979;236:H498–505. - PubMed
-
- Suga H, Sagawa K, Shoukas AA. Load independence of the instantaneous pressure-volume ratio of the canine left ventricle and effects of epinephrine and heart rate on the ratio. Circ Res. 1973;32:314–22. - PubMed
-
- Suga H, Sagawa K. Mathematical interrelationship between instantaneous ventricular pressure–volume ratio and myocardial force-velocity relation. Ann Biomed Eng. 1972;1:160–81. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources