

Sonographic markers for early diagnosis of fetal malformations
- PMID: 24179631
- PMCID: PMC3812447
- DOI: 10.4329/wjr.v5.i10.356
Sonographic markers for early diagnosis of fetal malformations
Abstract
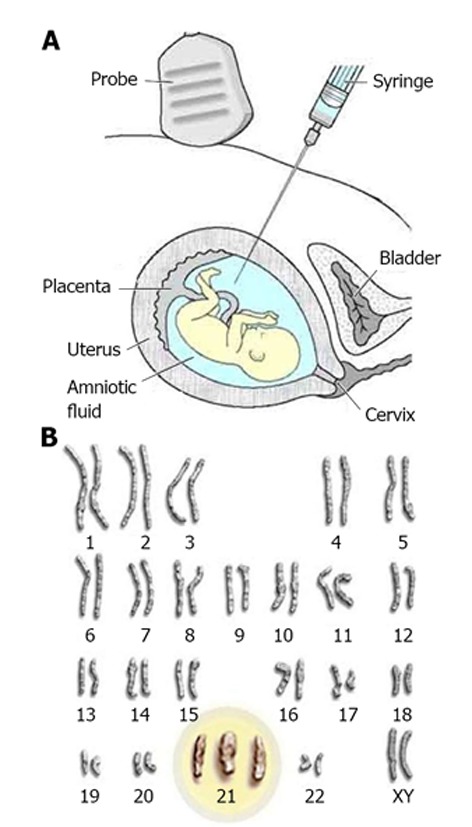
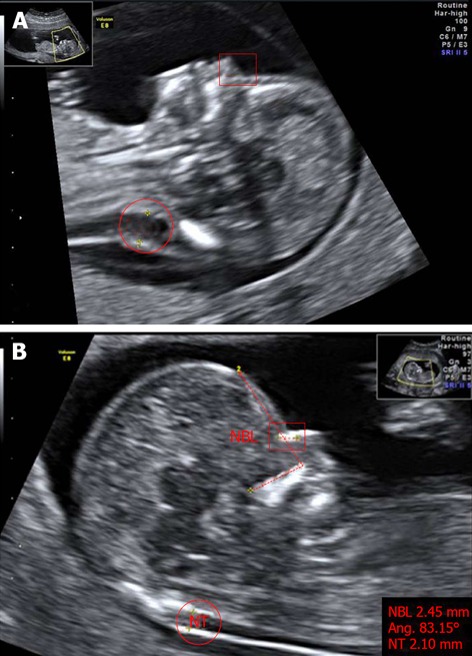
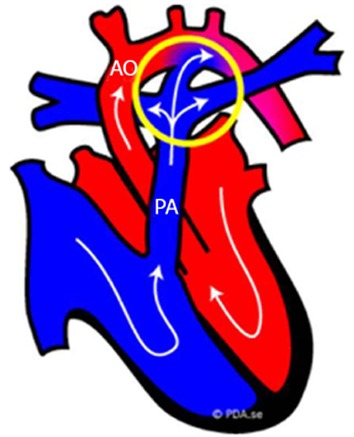
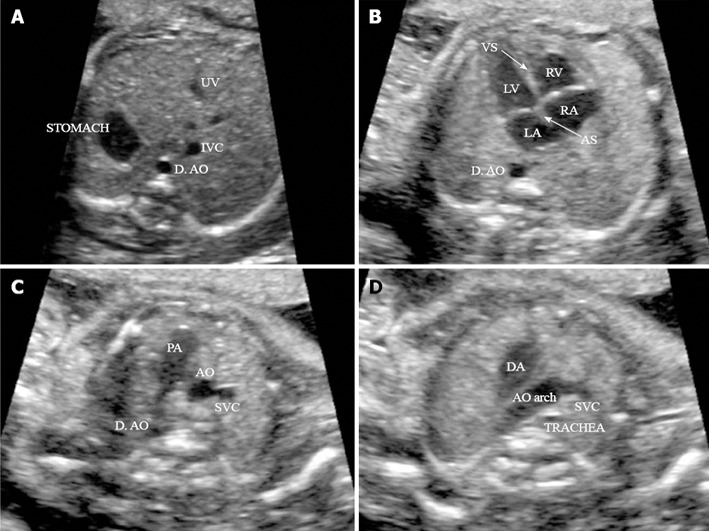
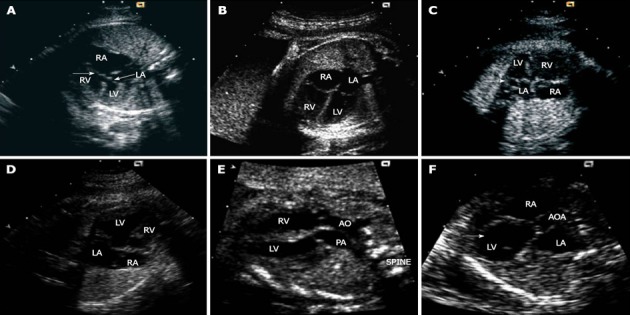
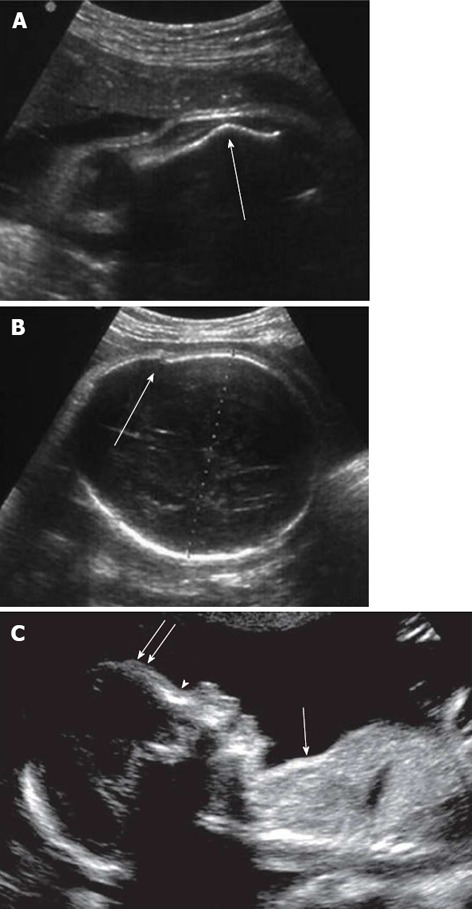
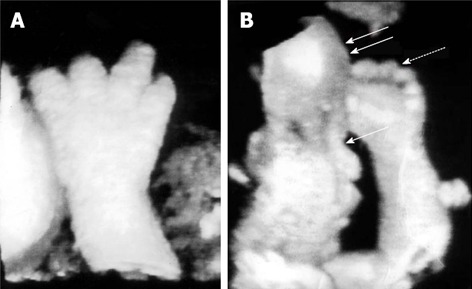
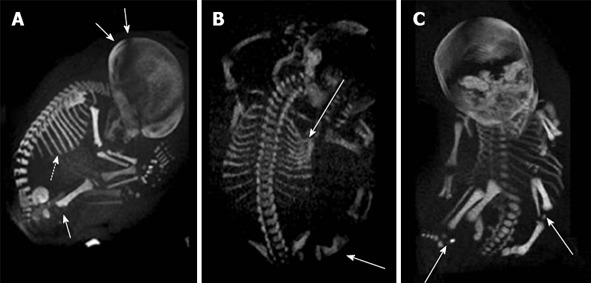
Fetal malformations are very frequent in industrialized countries. Although advanced maternal age may affect pregnancy outcome adversely, 80%-90% of fetal malformations occur in the absence of a specific risk factor for parents. The only effective approach for prenatal screening is currently represented by an ultrasound scan. However, ultrasound methods present two important limitations: the substantial absence of quantitative parameters and the dependence on the sonographer experience. In recent years, together with the improvement in transducer technology, quantitative and objective sonographic markers highly predictive of fetal malformations have been developed. These markers can be detected at early gestation (11-14 wk) and generally are not pathological in themselves but have an increased incidence in abnormal fetuses. Thus, prenatal ultrasonography during the second trimester of gestation provides a "genetic sonogram", including, for instance, nuchal translucency, short humeral length, echogenic bowel, echogenic intracardiac focus and choroid plexus cyst, that is used to identify morphological features of fetal Down's syndrome with a potential sensitivity of more than 90%. Other specific and sensitive markers can be seen in the case of cardiac defects and skeletal anomalies. In the future, sonographic markers could limit even more the use of invasive and dangerous techniques of prenatal diagnosis (amniocentesis, etc.).
Keywords: Chromosome abnormalities; Fetal echocardiography; Nuchal translucency; Prenatal diagnosis; Prenatal sonography; Skeletal dysplasia.
Figures
Similar articles
-
The use of second-trimester genetic sonogram in guiding clinical management of patients at increased risk for fetal trisomy 21.Obstet Gynecol. 1996 Jun;87(6):948-52. doi: 10.1016/0029-7844(96)00053-1. Obstet Gynecol. 1996. PMID: 8649704
-
[Second trimester sonographic screening for Down's syndrome and other chromosomal abnormalities].Akush Ginekol (Sofiia). 2002;41(5):7-19. Akush Ginekol (Sofiia). 2002. PMID: 12440332 Bulgarian.
-
Age-adjusted ultrasound risk assessment for fetal Down's syndrome during the second trimester: description of the method and analysis of 142 cases.Ultrasound Obstet Gynecol. 1998 Jul;12(1):8-14. doi: 10.1046/j.1469-0705.1998.12010008.x. Ultrasound Obstet Gynecol. 1998. PMID: 9697277
-
Sonographic markers of fetal trisomies: second trimester.J Ultrasound Med. 2001 Jun;20(6):655-74. doi: 10.7863/jum.2001.20.6.655. J Ultrasound Med. 2001. PMID: 11400940 Review.
-
Diagnosis and management of fetal nuchal translucency.Semin Roentgenol. 1998 Oct;33(4):333-8. doi: 10.1016/s0037-198x(98)80040-0. Semin Roentgenol. 1998. PMID: 9800243 Review.
Cited by
-
"Down syndrome: an insight of the disease".J Biomed Sci. 2015 Jun 11;22(1):41. doi: 10.1186/s12929-015-0138-y. J Biomed Sci. 2015. PMID: 26062604 Free PMC article. Review.
-
Evaluation of the Association between Fetal Cardiac Disorders with Choroid Plexus Cyst in Fetuses.J Cardiovasc Dev Dis. 2022 Feb 16;9(2):60. doi: 10.3390/jcdd9020060. J Cardiovasc Dev Dis. 2022. PMID: 35200713 Free PMC article.
-
Cardiac Axis in Early Gestation and Congenital Heart Disease.Curr Cardiol Rev. 2024 Jan 24;20(1):E240124226100. doi: 10.2174/011573403X264660231210162041. Online ahead of print. Curr Cardiol Rev. 2024. PMID: 38279755 Free PMC article.
-
Quantitative analysis of total β-subunit of human chorionic gonadotropin concentration in urine by immunomagnetic reduction to assist in the diagnosis of ectopic pregnancy.Int J Nanomedicine. 2015 Mar 30;10:2475-83. doi: 10.2147/IJN.S81201. eCollection 2015. Int J Nanomedicine. 2015. PMID: 25848265 Free PMC article.
-
Effectiveness of Chromosomal Microarray Analysis for Prenatal Diagnosis of Fetal Echogenic Intracardiac Focus: A Single-Center Experience.Int J Gen Med. 2021 May 21;14:1991-1997. doi: 10.2147/IJGM.S311800. eCollection 2021. Int J Gen Med. 2021. PMID: 34045891 Free PMC article.
References
-
- Kouamé N, N’goan-Domoua AM, Nikiéma Z, Konan AN, N’guessan KE, Sétchéou A, Tra-Bi ZO, N’gbesso RD, Kéita AK. Polyhydramnios: a warning sign in the prenatal ultrasound diagnosis of foetal malformation? Diagn Interv Imaging. 2013;94:433–437. - PubMed
-
- Katorza E, Achiron R. Early pregnancy scanning for fetal anomalies--the new standard? Clin Obstet Gynecol. 2012;55:199–216. - PubMed
-
- Fong KW, Toi A, Salem S, Hornberger LK, Chitayat D, Keating SJ, McAuliffe F, Johnson JA. Detection of fetal structural abnormalities with US during early pregnancy. Radiographics. 2004;24:157–174. - PubMed
-
- Stoll C, Clementi M. Prenatal diagnosis of dysmorphic syndromes by routine fetal ultrasound examination across Europe. Ultrasound Obstet Gynecol. 2003;21:543–551. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
