

Renal medullary carcinoma response to chemotherapy: a referral center experience in Brazil
- PMID: 24179656
- PMCID: PMC3804819
- DOI: 10.4081/rt.2013.e44
Renal medullary carcinoma response to chemotherapy: a referral center experience in Brazil
Abstract
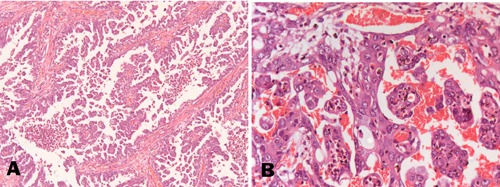
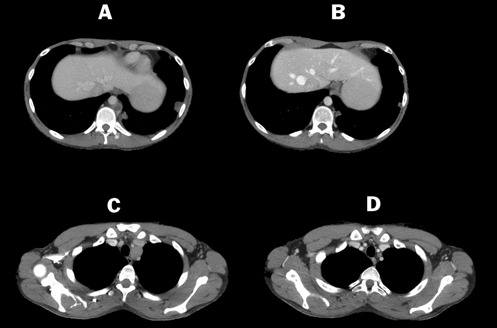
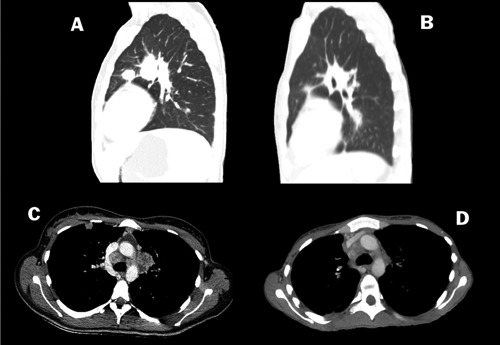
Renal medullary carcinoma (RMC) is rare, accounting for less than 1% of all renal neoplasms. Case reports suggest RMC is highly aggressive, poorly responsive to chemotherapy, often metastatic at diagnosis, affects young men with sickle cell trait, and median overall survival (mOS) is less than 12 months. We report the epidemiological characteristics, treatments performed, response rate to each treatment and mOS of five patients with RMC. All patients had sickle cell trait, four were male, three had metastatic disease at diagnosis and mean age at diagnosis was 25 years. Non-metastatic patients were submitted to nephrectomy. Two patients had partial response to first line chemotherapy including cisplatin and gemcitabine. There was no response to sunitinib or second line chemo - therapy; mOS was 6 months. Due to its rarity, case series are the only evidence available to discuss the treatment for RMC. In our experience, only cisplatin and gemcitabine based regimen offered response.
Keywords: carcinoma; kidney neoplasms; renal cell; renal medullary carcinoma; sickle cell trait.
Figures
References
-
- Hakimi AA, Koi PT, Milhoua PM, et al. Renal medullary carcinoma: the Bronx experience. Urology 2007;70:878-82 - PubMed
-
- Davis CJ, Jr, Mostofi FK, Sesterhenn IA.Renal medullary carcinoma. The seventh sickle cell nephropathy. Am J Surg Pathol 1995;19:1-11 - PubMed
-
- Swartz MA, Karth J, Schneider DT, et al. Renal medullary carcinoma: clinical, pathologic, immunohistochemical, and genetic analysis with pathogenetic implications. Urology 2002;60:1083-9 - PubMed
-
- Strouse JJ, Spevak M, Mack AK, et al. Significant responses to platinum-based chemotherapy in renal medullary carcinoma. Pediatr Blood Cancer 2005;44:407-11 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
