

Frailty and risk in proximal aortic surgery
- PMID: 24183336
- PMCID: PMC4336171
- DOI: 10.1016/j.jtcvs.2013.09.011
Frailty and risk in proximal aortic surgery
Abstract
Objectives: Although frailty has recently been examined in various populations as a predictor of morbidity and mortality, its effect on thoracic aortic surgery outcomes has not been studied. The objective of the present study was to evaluate the role of frailty in predicting postoperative morbidity and mortality in patients undergoing proximal aortic replacement surgery.
Methods: A retrospective analysis of a prospectively maintained database was performed for all patients undergoing elective and nonelective proximal aortic operations (root, ascending aorta, and/or arch) at a single-referral institution from June 2005 to December 2012. A total of 581 patients underwent proximal aortic surgery, of whom 574 (98.8%) were included in the present analysis; 7 were excluded because of incomplete data. Frailty was evaluated using an index consisting of age >70 years, body mass index <18.5 kg/m(2), anemia, history of stroke, hypoalbuminemia, and total psoas volume in the bottom quartile of the population. One point was given for each criterion met to determine a frailty score of 0 to 6. Frailty was defined as a score of ≥2. Risk models for length of stay >14 days, discharge to other than home, 30-day composite major morbidity, 30-day composite major morbidity/mortality, and 30-day and 1-year mortality were calculated using multivariate regression modeling.
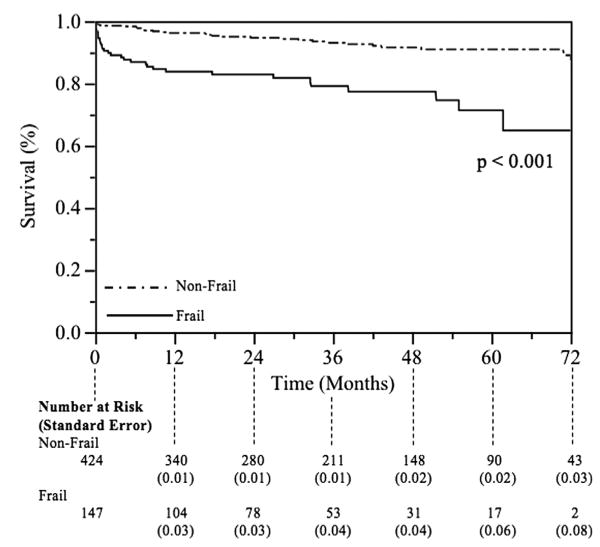
Results: Of the 574 patients, 148 (25.7%) were defined as frail (frailty score ≥2). The unadjusted 30-day/in-hospital and long-term outcomes were significantly worse for the frail versus nonfrail patients in all but 1 of the outcomes analyzed; no difference was found in the 30-day readmission rates between the 2 groups. In the multivariate model, a frailty score of ≥2 was associated with discharge to other than home and 30-day and 1-year mortality.
Conclusions: Frailty, as defined using a 6-component frailty index, can serve as an independent predictor of discharge disposition and early and late mortality risk in patients undergoing proximal aortic surgery. These frailty markers, all of which are easily assessed preoperatively, could provide valuable information for patient counseling and risk stratification before proximal aortic replacement.
Keywords: 26.1; FP; NFP; STS; TPV; The Society of Thoracic Surgeons; frail patient; nonfrail patient; total psoas volume.
Copyright © 2014 The American Association for Thoracic Surgery. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Krahenbuhl ES, Immer FF, Stalder M, Englberger L, Eckstein FS, Schmidli J, et al. Technical advances improved outcome in patients undergoing surgery of the ascending aorta and/or aortic arch: ten years' experience. Eur J Cardiothorac Surg. 2008;34:595–9. - PubMed
-
- Chikwe J, Adams DH. Frailty: the missing element in predicting operative mortality. Semin Thorac Cardiovasc Surg. 2010;22:109–10. - PubMed
-
- [Accessed June 14, 2013];Adult Cardiac Surgery Database Training Manual version 2.73, 2012. Available at: http://www.sts.org/sites/default/files/documents/Training Manual Update 8 12.pdf.
-
- Lee DH, Buth KJ, Martin BJ, Yip AM, Hirsch GM. Frail patients are at increased risk for mortality and prolonged institutional care after cardiac surgery. Circulation. 2010;121:973–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
