

Health-related quality of life in patients with autosomal dominant polycystic kidney disease and CKD stages 1-4: a cross-sectional study
- PMID: 24183837
- PMCID: PMC4075014
- DOI: 10.1053/j.ajkd.2013.08.017
Health-related quality of life in patients with autosomal dominant polycystic kidney disease and CKD stages 1-4: a cross-sectional study
Abstract
Background: In people with early autosomal dominant polycystic kidney disease (ADPKD), average total kidney volume (TKV) is 3 times normal and increases by an average of 5% per year despite a seemingly normal glomerular filtration rate (GFR). We hypothesized that increased TKV would be a source of morbidity and diminished quality of life that would be worse in patients with more advanced disease.
Study design: Cross-sectional.
Setting & participants: 1,043 patients with ADPKD, hypertension, and a baseline estimated GFR (eGFR)> 20mL/min/1.73m(2).
Predictors: (1) eGFR, (2) height-adjusted TKV (htTKV) in patients with eGFR> 60mL/min/1.73m(2).
Outcomes: 36-Item Short Form Health Survey (SF-36) and the Wisconsin Brief Pain Survey.
Measurements: Questionnaires were self-administered. GFR was estimated from serum creatinine using the CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) equation. htTKV was measured by magnetic resonance imaging.
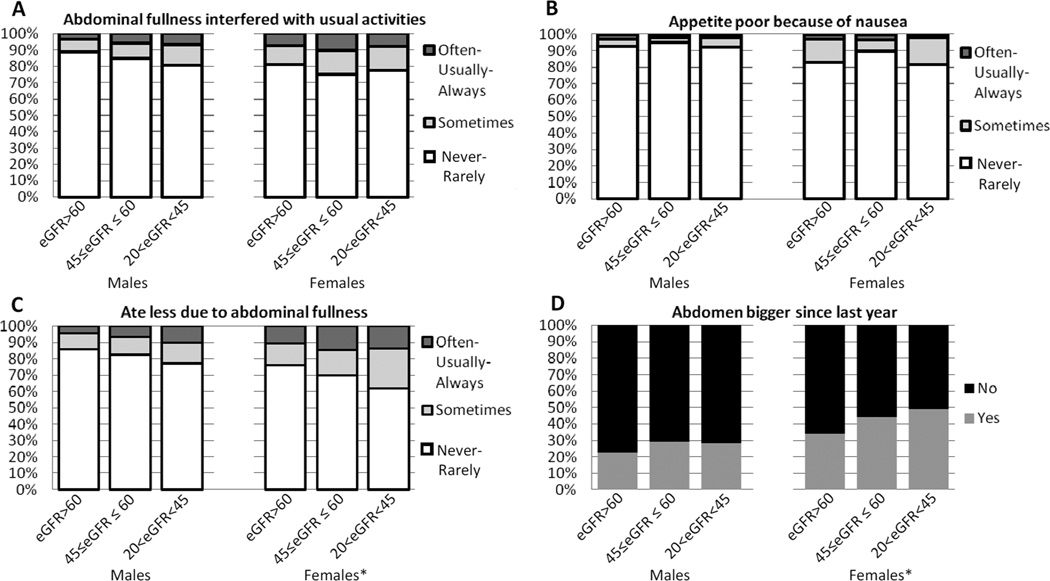
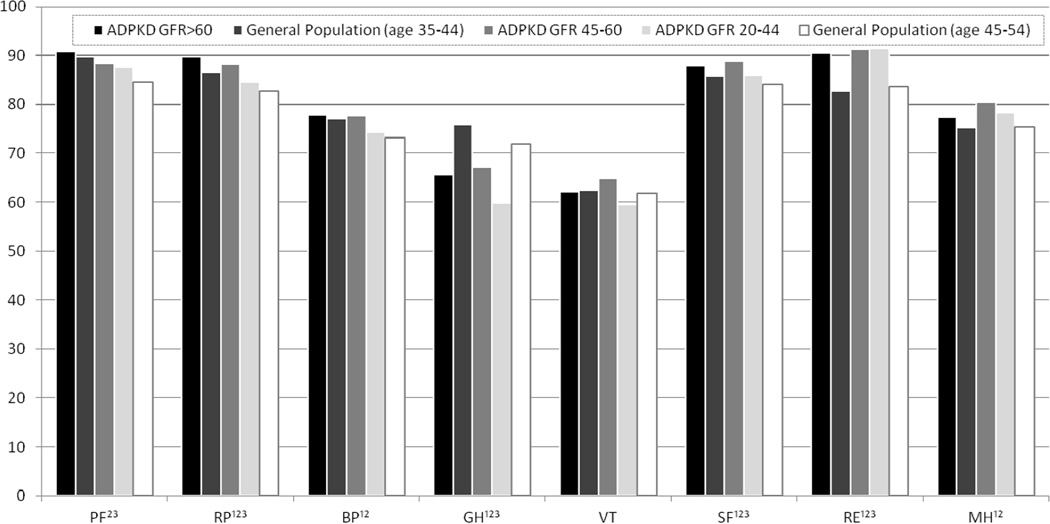
Results: Back pain was reported by 50% of patients, and 20% experienced it "often, usually, or always." In patients with early disease (eGFR> 60mL/min/1.73m(2)), there was no association between pain and htTKV, except in patients with large kidneys (htTKV> 1,000mL/m). Comparing across eGFR levels and including patients with eGFRs< 60mL/min/1.73m(2), patients with eGFRs of 20-44mL/min/1.73m(2) were significantly more likely to report that pain impacted on their daily lives and had lower SF-36 scores than patients with eGFRs of 45-60 and ≥60mL/min/1.73m(2). Symptoms relating to abdominal fullness were reported by 20% of patients and were related significantly to lower eGFRs in women, but not men.
Limitations: TKV and liver volume were not measured in patients with eGFR < 60mL/min/1.73m(2). The number of patients with eGFRs< 30mL/min/1.73m(2) is small. Causal inferences are limited by cross-sectional design.
Conclusions: Pain is a common early symptom in the course of ADPKD, although it is not related to kidney size in early disease (eGFR> 60mL/min/1.73m(2)), except in individuals with large kidneys (htTKV> 1,000 mL/m). Symptoms relating to abdominal fullness and pain are greater in patients with more advanced (eGFR, 20-45mL/min/1.73m(2)) disease and may be due to organ enlargement, especially in women. More research about the role of TKV in quality of life and outcomes of patients with ADPKD is warranted.
Keywords: Autosomal dominant polycystic kidney disease (ADPKD); activities of daily life; chronic kidney disease (CKD); extrarenal symptoms; patient-reported outcomes; quality of life (QoL); renal disease.
Copyright © 2014 National Kidney Foundation, Inc. All rights reserved.
Conflict of interest statement
N SECTION: Because a quorum could not be reached after those editors with potential conflicts recused themselves from consideration of this manuscript, the peer-review and decision-making processes were handled entirely by an Associate Editor (Kamyar Kalantar-Zadeh, MD, MPH, PhD) who served as Acting Editor-in-Chief. Details of the journal’s procedures for potential editor conflicts are given in the Editorial Policies section of the AJKD website.
Figures
References
-
- Gabow PA. Autosomal dominant polycystic kidney disease. New Engl J Med. 1993;329(5):332–342. - PubMed
-
- Granthum JJ, Chapman AB, T VE. Volume Progression in Autosomal Dominant Polycystic Kidney Disease: The Major Factor Determining Clinical Outcomes. Clin J Am Soc Nephrol. 2006;1:148–157. - PubMed
-
- Bajwa ZH, Gupta S, Warfield CA, S TI. Pain management in polycystic kidney disease. Kidney Int. 2001;60(5):1631–1644. - PubMed
-
- Grantham JJ, Torres VE, Chapman AB, Guay-Woodford LM, Bae KT, King BF, Wetzel LH, Baumgarten DA, Kenney PJ, Harris PC, Klahr S, Bennett WM, Hirschman GN, Meyers CM, Zhang X, Zhu F, Miller JP. Volume progression in polycystic kidney disease. New Engl J Med. 2006;354(20):2122–2130. - PubMed
-
- Serra AL, Poster D, Kistler AD, Krauer F, Raina S, Young J, Rentsch KM, Spanaus KS, Senn O, Kristanto P, Scheffel H, Weishaupt D, W RP. Sirolimus and Kidney Growth in Autosomal Dominant Polycystic Kidney Disease. New Engl J Med. 2010;363:820–829. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 DK056956/DK/NIDDK NIH HHS/United States
- P30 DK090728/DK/NIDDK NIH HHS/United States
- U01 DK062402/DK/NIDDK NIH HHS/United States
- DK62410/DK/NIDDK NIH HHS/United States
- UL1 RR025752/RR/NCRR NIH HHS/United States
- DK62402/DK/NIDDK NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- M01 RR000051/RR/NCRR NIH HHS/United States
- U01 DK062411/DK/NIDDK NIH HHS/United States
- UL1 TR001082/TR/NCATS NIH HHS/United States
- RR024150/RR/NCRR NIH HHS/United States
- RR025752/RR/NCRR NIH HHS/United States
- RR23940/RR/NCRR NIH HHS/United States
- RR00585/RR/NCRR NIH HHS/United States
- U01 DK062401/DK/NIDDK NIH HHS/United States
- M01 RR000585/RR/NCRR NIH HHS/United States
- UL1 RR024989/RR/NCRR NIH HHS/United States
- DK62401/DK/NIDDK NIH HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- M01 RR000039/RR/NCRR NIH HHS/United States
- RR024296/RR/NCRR NIH HHS/United States
- M01 RR000054/RR/NCRR NIH HHS/United States
- M01 RR023940/RR/NCRR NIH HHS/United States
- RR024989/RR/NCRR NIH HHS/United States
- DK62408/DK/NIDDK NIH HHS/United States
- RR000054/RR/NCRR NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- U01 DK062408/DK/NIDDK NIH HHS/United States
- U01 DK082230/DK/NIDDK NIH HHS/United States
- UL1 RR024150/RR/NCRR NIH HHS/United States
- RR000039/RR/NCRR NIH HHS/United States
- UL1 RR025008/RR/NCRR NIH HHS/United States
- RR025780/RR/NCRR NIH HHS/United States
- DK62411/DK/NIDDK NIH HHS/United States
- U01 DK062410/DK/NIDDK NIH HHS/United States
- RR025008/RR/NCRR NIH HHS/United States
- RR000051/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
