

Impaired systolic function by strain imaging in heart failure with preserved ejection fraction
- PMID: 24184245
- PMCID: PMC7195816
- DOI: 10.1016/j.jacc.2013.09.052
Impaired systolic function by strain imaging in heart failure with preserved ejection fraction
Erratum in
- J Am Coll Cardiol. 2014 Jul 22;64(3):335
Abstract
Objectives: This study sought to determine the frequency and magnitude of impaired systolic deformation in heart failure with preserved ejection fraction (HFpEF).
Background: Although diastolic dysfunction is widely considered a key pathophysiologic mediator of HFpEF, the prevalence of concomitant systolic dysfunction has not been clearly defined.
Methods: We assessed myocardial systolic and diastolic function in 219 HFpEF patients from a contemporary HFpEF clinical trial. Myocardial deformation was assessed using a vendor-independent 2-dimensional speckle-tracking software. The frequency and severity of impaired deformation was assessed in HFpEF, and compared to 50 normal controls free of cardiovascular disease and to 44 age- and sex-matched hypertensive patients with diastolic dysfunction (hypertensive heart disease) but no HF. Among HFpEF patients, clinical, echocardiographic, and biomarker correlates of left ventricular strain were determined.
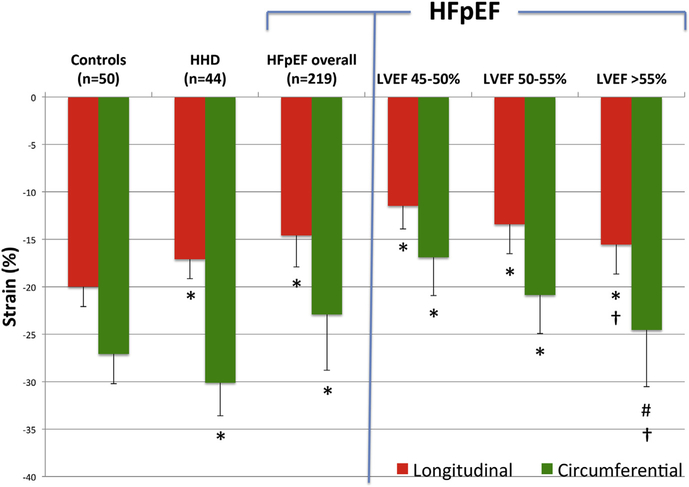
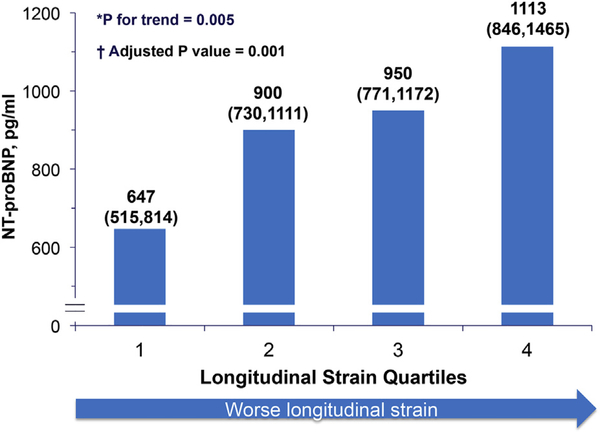
Results: The HFpEF patients had preserved left ventricular ejection fraction and evidence of diastolic dysfunction. Compared to both normal controls and hypertensive heart disease patients, the HFpEF patients demonstrated significantly lower longitudinal strain (LS) (-20.0 ± 2.1 and -17.07 ± 2.04 vs. -14.6 ± 3.3, respectively, p < 0.0001 for both) and circumferential strain (CS) (-27.1 ± 3.1 and -30.1 ± 3.5 vs. -22.9 ± 5.9, respectively; p < 0.0001 for both). In HFpEF, both LS and CS were related to LVEF (LS, R = -0.46; p < 0.0001; CS, R = -0.51; p < 0.0001) but not to standard echocardiographic measures of diastolic function (E' or E/E'). Lower LS was modestly associated with higher NT-proBNP, even after adjustment for 10 baseline covariates including LVEF, measures of diastolic function, and LV filling pressure (multivariable adjusted p = 0.001).
Conclusions: Strain imaging detects impaired systolic function despite preserved global LVEF in HFpEF that may contribute to the pathophysiology of the HFpEF syndrome. (LCZ696 Compared to Valsartan in Patients With Chronic Heart Failure and Preserved Left-ventricular Ejection Fraction; NCT00887588).
Keywords: CS; HF; HFpEF; HHD; LA; LAVi; LS; LV; LVEF; N-terminal pro-brain natriuretic peptide; NT-proBNP; RWT; cardiac biomarkers; circumferential strain; diastolic heart failure; echocardiography; heart failure; heart failure with preserved ejection fraction; hypertensive heart disease; left atrial; left atrial volume index; left ventricular; left ventricular ejection fraction; longitudinal strain; mechanics; relative wall thickness; systolic strain.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Heart failure with preserved ejection fraction: a heterogenous disorder with multifactorial pathophysiology.J Am Coll Cardiol. 2014 Feb 11;63(5):457-9. doi: 10.1016/j.jacc.2013.10.007. Epub 2013 Oct 30. J Am Coll Cardiol. 2014. PMID: 24184240 Free PMC article. No abstract available.
-
Does speckle tracking really improve diagnosis and risk stratification in patients with HF with normal EF?J Am Coll Cardiol. 2014 Oct 7;64(14):1535. doi: 10.1016/j.jacc.2014.02.616. J Am Coll Cardiol. 2014. PMID: 25277623 No abstract available.
-
Reply: does speckle tracking really improve diagnosis and risk stratification in patients with HF with normal EF?J Am Coll Cardiol. 2014 Oct 7;64(14):1535-6. doi: 10.1016/j.jacc.2014.04.084. J Am Coll Cardiol. 2014. PMID: 25277624 No abstract available.
References
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006;355:251–9. - PubMed
-
- Owan TE, Redfield MM. Epidemiology of diastolic heart failure. Prog Cardiovasc Dis 2005;47:320–32. - PubMed
-
- Paulus WJ, Tschoepe C, Sanderson JE, et al. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure Echocardiography Associations of the European Society of Cardiology. Eur Heart J 2007;28:2539–50. - PubMed
-
- Zile MR, Baicu CF, Gaasch WH. Diastolic heart failure—abnormalities inactiverelaxationandpassivestiffnessoftheleftventricle.NEnglJMed 2004;350:1953–9. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
