

The influence of anesthesia and pain management on cognitive dysfunction after joint arthroplasty: a systematic review
- PMID: 24186470
- PMCID: PMC3971229
- DOI: 10.1007/s11999-013-3363-2
The influence of anesthesia and pain management on cognitive dysfunction after joint arthroplasty: a systematic review
Abstract
Background: Despite the overall success of total joint arthroplasty, patients undergoing this procedure remain susceptible to cognitive decline and/or delirium, collectively termed postoperative cognitive dysfunction. However, no consensus exists as to whether general or regional anesthesia results in a lower likelihood that a patient may experience this complication, and controversy surrounds the role of pain management strategies to minimize the incidence of postoperative cognitive dysfunction.
Questions/purposes: We systematically reviewed the English-language literature to assess the influence of the following anesthetic and/or pain management strategies on the risk for postoperative cognitive dysfunction in patients undergoing elective joint arthroplasty: (1) general versus regional anesthesia, (2) different parenteral, neuraxial, or inhaled agents within a given type of anesthetic (general or regional), (3) multimodal anesthetic techniques, and (4) different postoperative pain management regimens.
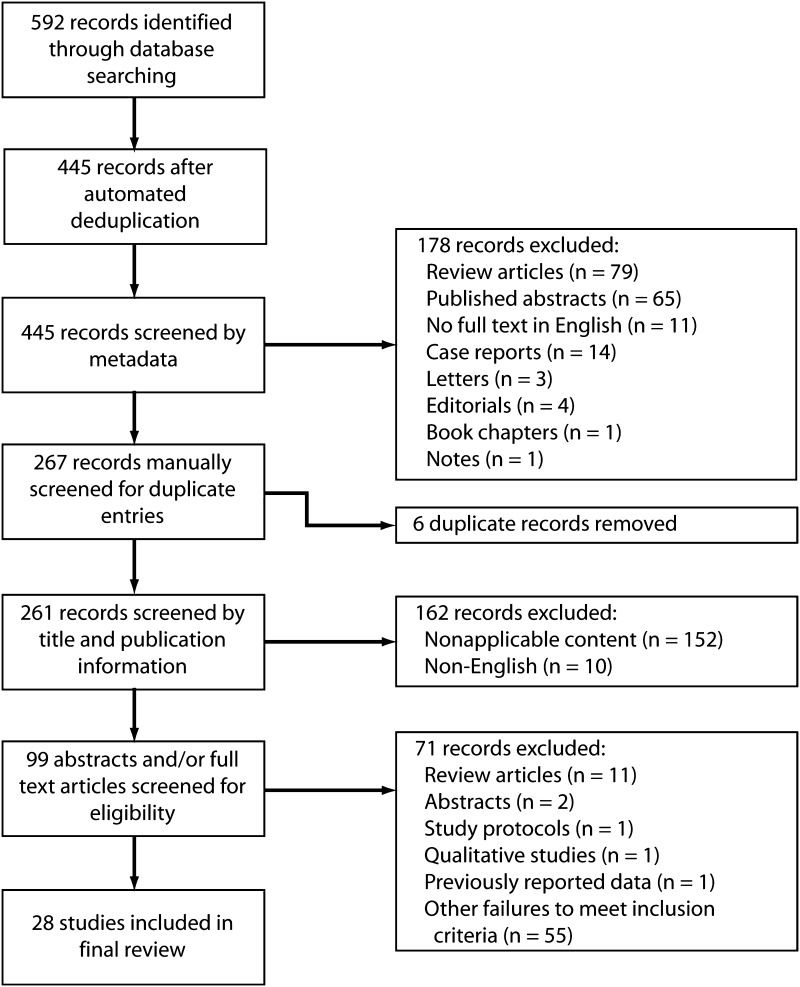
Methods: A systematic search was performed of the MEDLINE(®) and EMBASE™ databases to identify all studies that assessed the influence of anesthetic and/or pain management strategies on the risk for postoperative cognitive dysfunction after elective joint arthroplasty. Twenty-eight studies were included in the final review, of which 21 (75%) were randomized controlled (Level I) trials, two (7%) were prospective comparative (Level II) studies, two (7%) used a case-control (Level III) design, and three (11%) used retrospective comparative (Level III) methodology.
Results: The evidence published to date suggests that general anesthesia may be associated with increased risk of early postoperative cognitive dysfunction in the early postoperative period as compared to regional anesthesia, although this effect was not seen beyond 7 days. Optimization of depth of general anesthesia with comprehensive intraoperative cerebral monitoring may be beneficial, although evidence is equivocal. Multimodal anesthesia protocols have not been definitively demonstrated to reduce the incidence of postoperative cognitive dysfunction. Nonopioid postoperative pain management techniques, limiting narcotics to oral formulations and avoiding morphine, appear to reduce the risk of postoperative cognitive dysfunction.
Conclusions: Both anesthetic and pain management strategies appear to influence the risk of early cognitive dysfunction after elective joint arthroplasty, although only one study identified differences that persisted beyond 1 week after surgery. Investigators should strive to use accepted, validated tools for the assessment of postoperative cognitive dysfunction and to carefully report details of the anesthetic and analgesic techniques used in future studies.
Figures
References
-
- Diagnostic and Statistical Manual of Mental Health Disorders: DSM-5. Washington, DC: American Psychatric Publishing; 2013.
-
- Anwer HM, Swelem SE, El Sheshai A, Moustafa AA. Postoperative cognitive dysfunction in adult and elderly patients—general anesthesia vs subarachnoid or epidural analgesia. Middle East J Anesthesiol. 2006;18:1123–1138. - PubMed
-
- Ballard C, Jones E, Gauge N, Aarsland D, Nilsen OB, Saxby BK, Lowery D, Corbett A, Wesnes K, Katsaiti E, Arden J, Amoako D, Prophet N, Purushothaman B, Green D. Optimised anaesthesia to reduce post operative cognitive decline (POCD) in older patients undergoing elective surgery, a randomised controlled trial. PLoS One. 2012;7:e37410. doi: 10.1371/journal.pone.0037410. - DOI - PMC - PubMed
-
- Castellsague J, Riera-Guardia N, Calingaert B, Varas-Lorenzo C, Fourrier-Reglat A, Nicotra F, Sturkenboom M, Perez-Gutthann S. Individual NSAIDs and upper gastrointestinal complications: a systematic review and meta-analysis of observational studies (the SOS project) Drug Saf. 2012;35:1127–1146. doi: 10.1007/BF03261999. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
