

B-type natriuretic peptides and mortality after stroke: a systematic review and meta-analysis
- PMID: 24186915
- PMCID: PMC3854833
- DOI: 10.1212/01.wnl.0000436937.32410.32
B-type natriuretic peptides and mortality after stroke: a systematic review and meta-analysis
Abstract
Objective: To measure the association of B-type natriuretic peptide (BNP) and N-terminal fragment of BNP (NT-proBNP) with all-cause mortality after stroke, and to evaluate the additional predictive value of BNP/NT-proBNP over clinical information.
Methods: Suitable studies for meta-analysis were found by searching MEDLINE and EMBASE databases until October 26, 2012. Weighted mean differences measured effect size; meta-regression and publication bias were assessed. Individual participant data were used to estimate effects by logistic regression and to evaluate BNP/NT-proBNP additional predictive value by area under the receiver operating characteristic curves, and integrated discrimination improvement and categorical net reclassification improvement indexes.
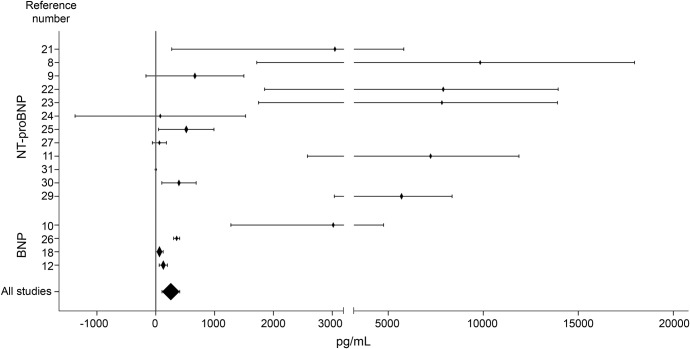
Results: Literature-based meta-analysis included 3,498 stroke patients from 16 studies and revealed that BNP/NT-proBNP levels were 255.78 pg/mL (95% confidence interval [CI] 105.10-406.47, p = 0.001) higher in patients who died; publication bias entailed the loss of this association. Individual participant data analysis comprised 2,258 stroke patients. After normalization of the data, patients in the highest quartile had double the risk of death after adjustment for clinical variables (NIH Stroke Scale score, age, sex) (odds ratio 2.30, 95% CI 1.32-4.01 for BNP; and odds ratio 2.63, 95% CI 1.75-3.94 for NT-proBNP). Only NT-proBNP showed a slight added value to clinical prognostic variables, increasing discrimination by 0.028 points (integrated discrimination improvement index; p < 0.001) and reclassifying 8.1% of patients into correct risk mortality categories (net reclassification improvement index; p = 0.003). Neither etiology nor time from onset to death affected the association of BNP/NT-proBNP with mortality.
Conclusion: BNPs are associated with poststroke mortality independent of NIH Stroke Scale score, age, and sex. However, their translation to clinical practice seems difficult because BNP/NT-proBNP add only minor predictive value to clinical information.
Figures


Comment in
-
Comment: Natriuretic peptides as predictive biomarkers of stroke outcome.Neurology. 2013 Dec 3;81(23):1983. doi: 10.1212/01.wnl.0000436941.55281.9c. Epub 2013 Nov 1. Neurology. 2013. PMID: 24186913 No abstract available.
-
Predicting stroke mortality: BNP could it be?Neurology. 2013 Dec 3;81(23):1970-1. doi: 10.1212/01.wnl.0000436949.75473.79. Epub 2013 Nov 1. Neurology. 2013. PMID: 24186914
-
B-type natriuretic peptides and mortality after stroke: a systematic review and meta-analysis.Neurology. 2014 Jul 15;83(3):292-3. doi: 10.1212/WNL.0000000000000634. Neurology. 2014. PMID: 25024445 No abstract available.
References
-
- Saposnik G, Kapral MK, Liu Y, et al. IScore: a risk score to predict death early after hospitalization for an acute ischemic stroke. Circulation 2011;123:739–749 - PubMed
-
- O'Donnell MJ, Fang J, D'Uva C, et al. The PLAN Score: a bedside prediction rule for death and severe disability following acute ischemic stroke. Arch Intern Med 2012;172:1548–1556 - PubMed
-
- Whiteley W, Chong WL, Sengupta A, Sandercock P. Blood markers for the prognosis of ischemic stroke: a systematic review. Stroke 2009;40:e380–e389 - PubMed
-
- deLemos JA, McGuire DK, Drazner MH. B-type natriuretic peptide in cardiovascular disease. Lancet 2003;362:316–322 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials