

Remodeling of the mononuclear phagocyte network underlies chronic inflammation and disease progression in heart failure: critical importance of the cardiosplenic axis
- PMID: 24186967
- PMCID: PMC5928520
- DOI: 10.1161/CIRCRESAHA.113.301720
Remodeling of the mononuclear phagocyte network underlies chronic inflammation and disease progression in heart failure: critical importance of the cardiosplenic axis
Abstract
Rationale: The role of mononuclear phagocytes in chronic heart failure (HF) is unknown.
Objective: Our aim was to delineate monocyte, macrophage, and dendritic cell trafficking in HF and define the contribution of the spleen to cardiac remodeling.
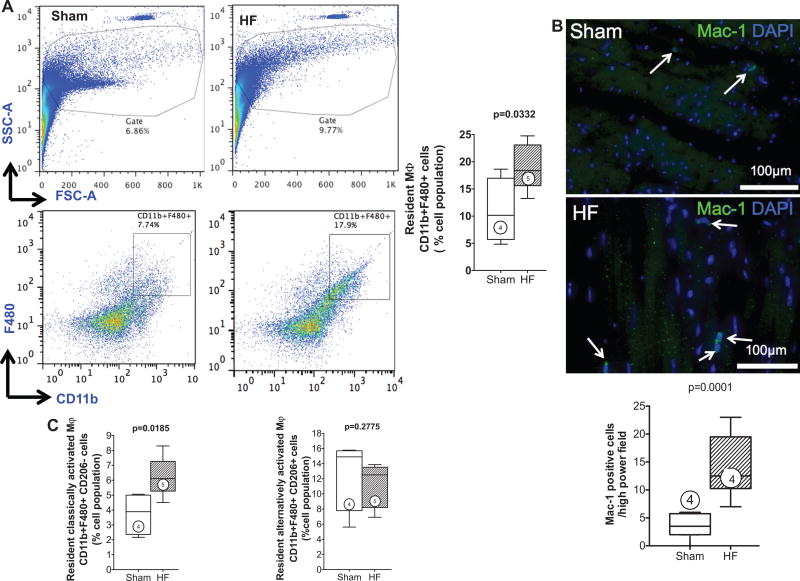
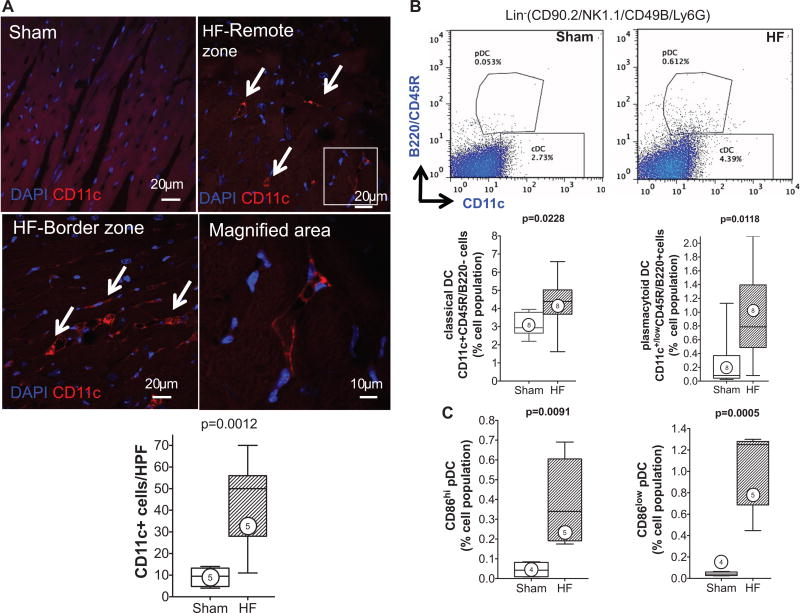
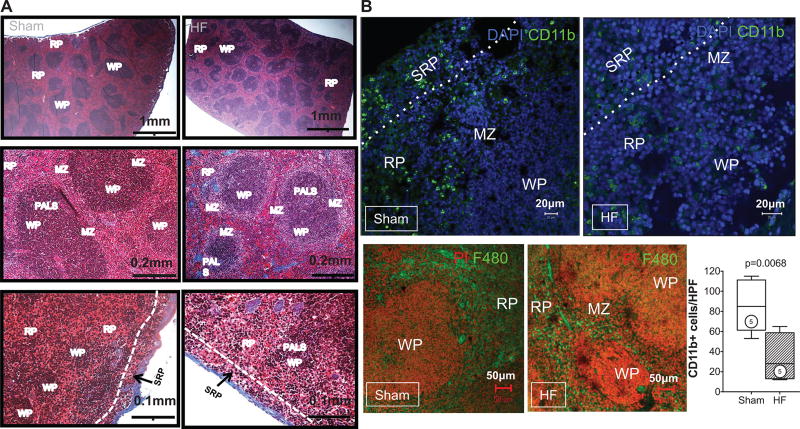
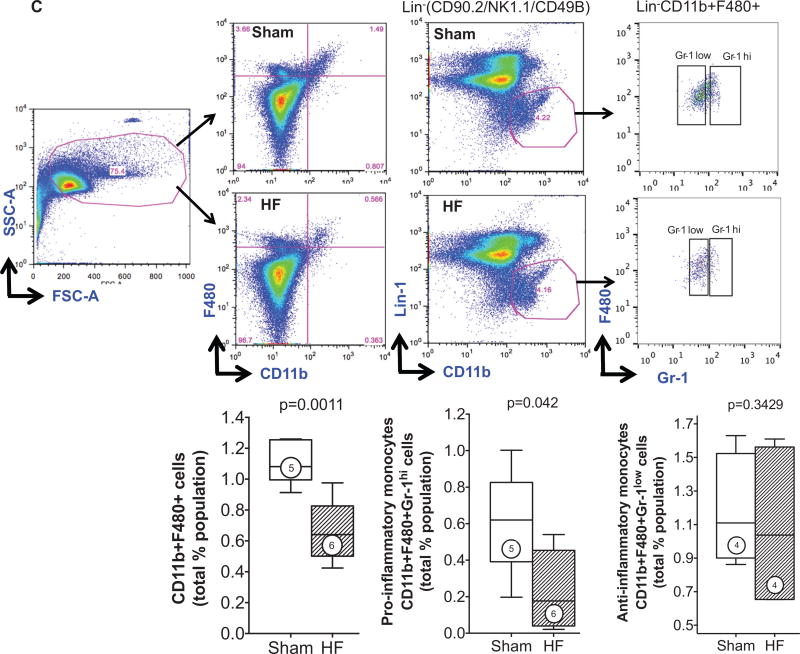
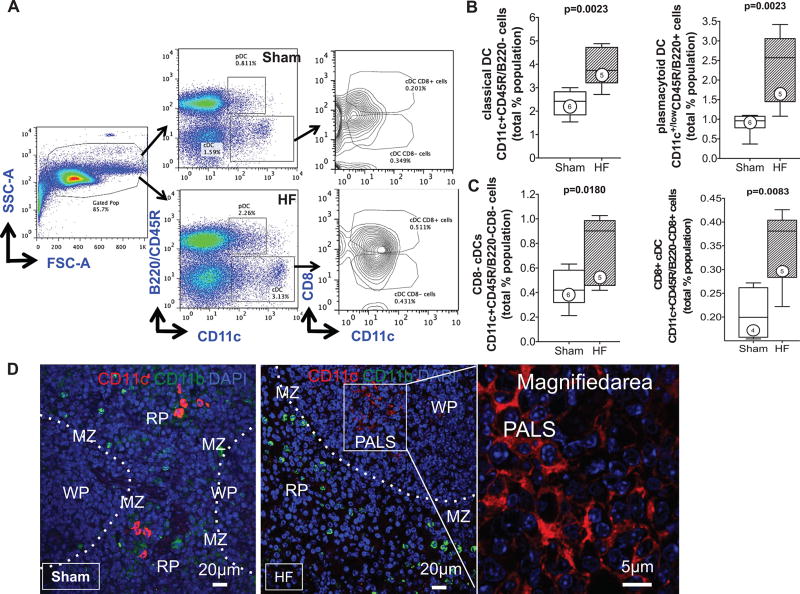
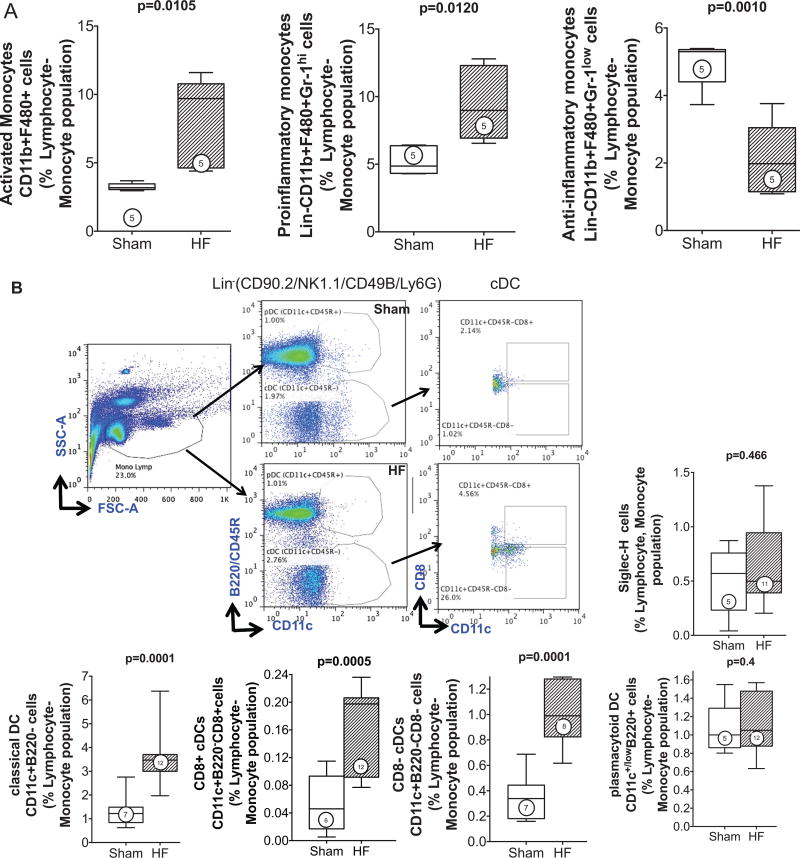
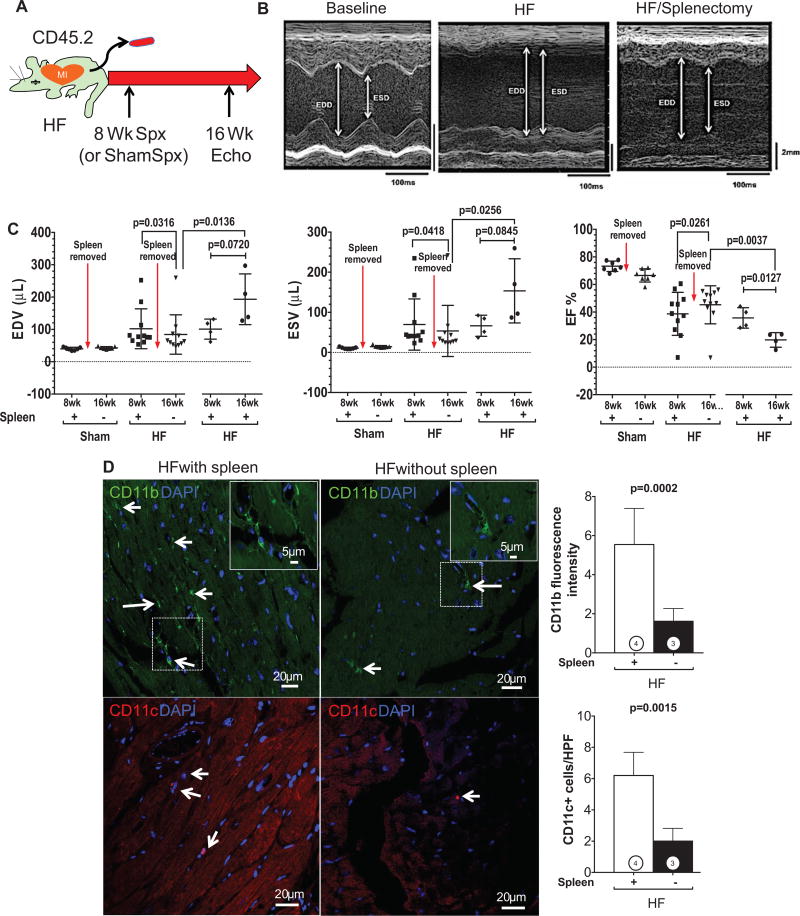
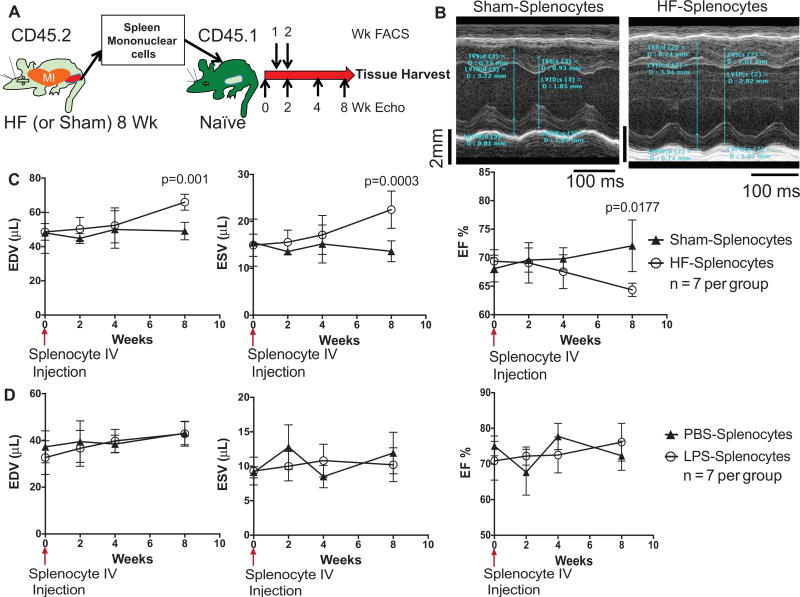
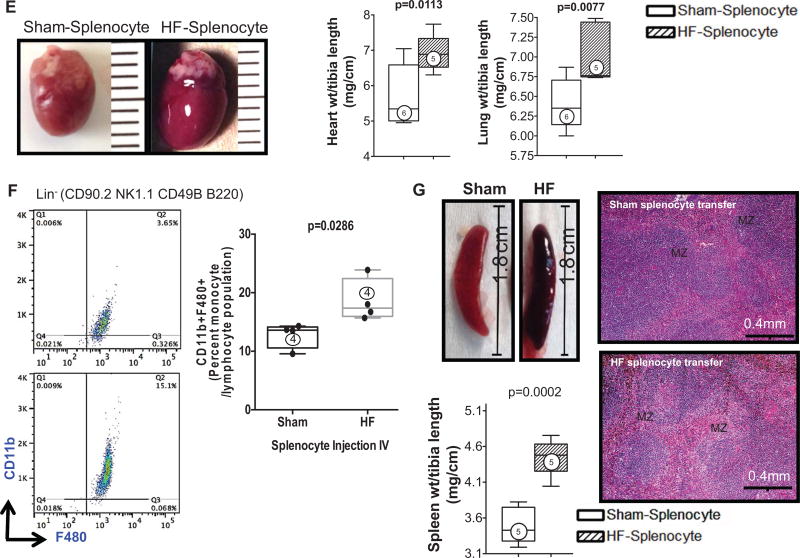
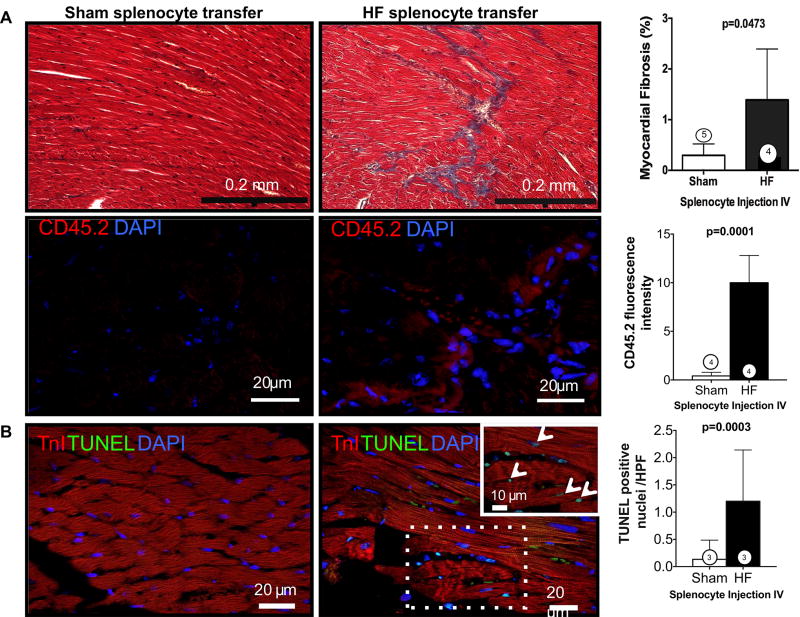
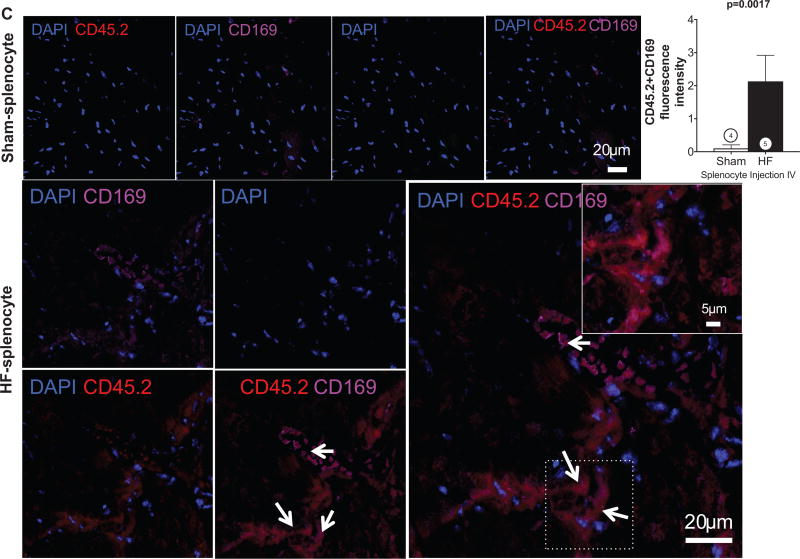
Methods and results: We evaluated C57Bl/6 mice with chronic HF 8 weeks after coronary ligation. As compared with sham-operated controls, HF mice exhibited: (1) increased proinflammatory CD11b+ F4/80+ CD206- macrophages and CD11b+ F4/80+ Gr-1(hi) monocytes in the heart and peripheral blood, respectively, and reduced CD11b+ F4/80+ Gr-1(hi) monocytes in the spleen; (2) significantly increased CD11c+ B220- classical dendritic cells and CD11c+ low)B220+ plasmacytoid dendritic cells in both the heart and spleen, and increased classic dendritic cells and plasmacytoid dendritic cells in peripheral blood and bone marrow, respectively; (3) increased CD4+ helper and CD8+ cytotoxic T-cells in the spleen; and (4) profound splenic remodeling with abundant white pulp follicles, markedly increased size of the marginal zone and germinal centers, and increased expression of alarmins. Splenectomy in mice with established HF reversed pathological cardiac remodeling and inflammation. Splenocytes adoptively transferred from mice with HF, but not from sham-operated mice, homed to the heart and induced long-term left ventricular dilatation, dysfunction, and fibrosis in naive recipients. Recipient mice also exhibited monocyte activation and splenic remodeling similar to HF mice.
Conclusions: Activation of mononuclear phagocytes is central to the progression of cardiac remodeling in HF, and heightened antigen processing in the spleen plays a critical role in this process. Splenocytes (presumably splenic monocytes and dendritic cells) promote immune-mediated injurious responses in the failing heart and retain this memory on adoptive transfer.
Keywords: dendritic cells; heart failure; inflammation; monocytes; spleen.
Figures
Comment in
-
Contribution of extramedullary organs in myocardial inflammation and remodeling: does the spleen cause cardiac melancholy?Circ Res. 2014 Jan 17;114(2):230-2. doi: 10.1161/CIRCRESAHA.113.302971. Circ Res. 2014. PMID: 24436423 Free PMC article. No abstract available.
References
-
- Mann DL. Inflammatory mediators and the failing heart: past, present, and the foreseeable future. Circ Res. 2002;91:988–998. - PubMed
-
- Bozkurt B, Mann DL, Deswal A. Biomarkers of inflammation in heart failure. Heart Fail Rev. 2010;15:331–341. - PubMed
-
- Braunwald E. Biomarkers in heart failure. N Engl J Med. 2008;358:2148–2159. - PubMed
-
- Prabhu SD. Cytokine-induced modulation of cardiac function. Circ Res. 2004;95:1140–1153. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
