

Gut-lung crosstalk in pulmonary involvement with inflammatory bowel diseases
- PMID: 24187454
- PMCID: PMC3812478
- DOI: 10.3748/wjg.v19.i40.6794
Gut-lung crosstalk in pulmonary involvement with inflammatory bowel diseases
Abstract
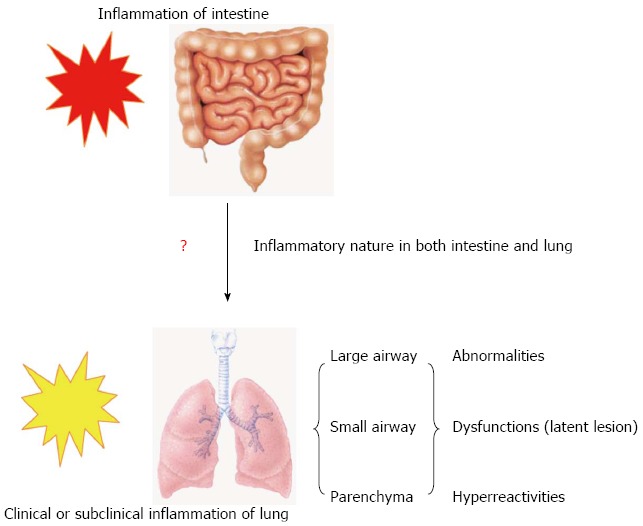
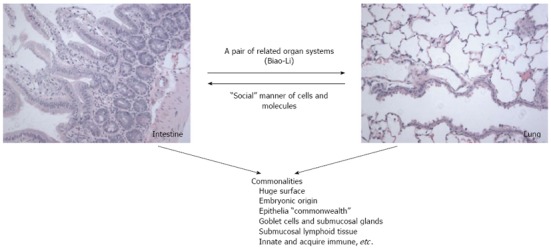
Pulmonary abnormalities, dysfunction or hyper-reactivity occurs in association with inflammatory bowel disease (IBD) more frequently than previously recognized. Emerging evidence suggests that subtle inflammation exists in the airways among IBD patients even in the absence of any bronchopulmonary symptoms, and with normal pulmonary functions. The pulmonary impairment is more pronounced in IBD patients with active disease than in those in remission. A growing number of case reports show that the IBD patients develop rapidly progressive respiratory symptoms after colectomy, with failure to isolate bacterial pathogens on repeated sputum culture, and often request oral corticosteroid therapy. All the above evidence indicates that the inflammatory changes in both the intestine and lung during IBD. Clinical or subclinical pulmonary inflammation accompanies the main inflammation of the bowel. Although there are clinical and epidemiological reports of chronic inflammation of the pulmonary and intestinal mucosa in IBD, the detailed mechanisms of pulmonary-intestinal crosstalk remain unknown. The lung has no anatomical connection with the main inflammatory site of the bowel. Why does the inflammatory process shift from the gastrointestinal tract to the airways? The clinical and subclinical pulmonary abnormalities, dysfunction, or hyper-reactivity among IBD patients need further evaluation. Here, we give an overview of the concordance between chronic inflammatory reactions in the airways and the gastrointestinal tract. A better understanding of the possible mechanism of the crosstalk among the distant organs will be beneficial in identifying therapeutic strategies for mucosal inflammatory diseases such as IBD and allergy.
Keywords: Biao-Li relationship; Gut-lung crosstalk; Inflammatory bowel disease; Pulmonary symptoms; Social manner.
Figures
Similar articles
-
Links Between Inflammatory Bowel Disease and Chronic Obstructive Pulmonary Disease.Front Immunol. 2020 Sep 11;11:2144. doi: 10.3389/fimmu.2020.02144. eCollection 2020. Front Immunol. 2020. PMID: 33042125 Free PMC article. Review.
-
Development, validation and implementation of an in vitro model for the study of metabolic and immune function in normal and inflamed human colonic epithelium.Dan Med J. 2015 Jan;62(1):B4973. Dan Med J. 2015. PMID: 25557335 Review.
-
Immunopathology of inflammatory bowel disease.World J Gastroenterol. 2014 Jan 7;20(1):6-21. doi: 10.3748/wjg.v20.i1.6. World J Gastroenterol. 2014. PMID: 24415853 Free PMC article. Review.
-
Pulmonary-intestinal cross-talk in mucosal inflammatory disease.Mucosal Immunol. 2012 Jan;5(1):7-18. doi: 10.1038/mi.2011.55. Epub 2011 Nov 16. Mucosal Immunol. 2012. PMID: 22089028 Free PMC article. Review.
-
Interaction Between Commensal Bacteria, Immune Response and the Intestinal Barrier in Inflammatory Bowel Disease.Front Immunol. 2021 Nov 11;12:761981. doi: 10.3389/fimmu.2021.761981. eCollection 2021. Front Immunol. 2021. PMID: 34858414 Free PMC article. Review.
Cited by
-
Gut Microbiota and SCFAs Play Key Roles in QingFei Yin Recipe Anti-Streptococcal Pneumonia Effects.Front Cell Infect Microbiol. 2021 Dec 7;11:791466. doi: 10.3389/fcimb.2021.791466. eCollection 2021. Front Cell Infect Microbiol. 2021. PMID: 34950611 Free PMC article.
-
Short-Chain Fatty Acid (SCFA) as a Connecting Link between Microbiota and Gut-Lung Axis-A Potential Therapeutic Intervention to Improve Lung Health.ACS Omega. 2024 Mar 19;9(13):14648-14671. doi: 10.1021/acsomega.3c05846. eCollection 2024 Apr 2. ACS Omega. 2024. PMID: 38585101 Free PMC article. Review.
-
Desired Turbulence? Gut-Lung Axis, Immunity, and Lung Cancer.J Oncol. 2017;2017:5035371. doi: 10.1155/2017/5035371. Epub 2017 Sep 17. J Oncol. 2017. PMID: 29075294 Free PMC article. Review.
-
Subclinical Pulmonary Involvement in Active IBD Responds to Biologic Therapy.J Crohns Colitis. 2021 Aug 2;15(8):1339-1345. doi: 10.1093/ecco-jcc/jjab024. J Crohns Colitis. 2021. PMID: 33544122 Free PMC article.
-
Dynamic Interplay Between Microbiota and Mucosal Immunity in Early Shaping of Asthma and its Implication for the COVID-19 Pandemic.J Asthma Allergy. 2020 Sep 28;13:369-383. doi: 10.2147/JAA.S272705. eCollection 2020. J Asthma Allergy. 2020. PMID: 33061464 Free PMC article. Review.
References
-
- Mudter J, Neurath MF. Insight into Crohn’s disease pathomorphology. Abdom Imaging. 2012;37:921–926. - PubMed
-
- Liu H, Patel NR, Walter L, Ingersoll S, Sitaraman SV, Garg P. Constitutive expression of MMP9 in intestinal epithelium worsens murine acute colitis and is associated with increased levels of proinflammatory cytokine Kc. Am J Physiol Gastrointest Liver Physiol. 2013;304:G793–G803. - PubMed
-
- Latella G, Fiocchi C, Caprili R. News from the “5th International Meeting on Inflammatory Bowel Diseases” CAPRI 2010. J Crohns Colitis. 2010;4:690–702. - PubMed
-
- Kappelman MD, Rifas-Shiman SL, Kleinman K, Ollendorf D, Bousvaros A, Grand RJ, Finkelstein JA. The prevalence and geographic distribution of Crohn’s disease and ulcerative colitis in the United States. Clin Gastroenterol Hepatol. 2007;5:1424–1429. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
