

Increased pelvic incidence may lead to arthritis and sagittal orientation of the facet joints at the lower lumbar spine
- PMID: 24188071
- PMCID: PMC4228336
- DOI: 10.1186/1471-2342-13-34
Increased pelvic incidence may lead to arthritis and sagittal orientation of the facet joints at the lower lumbar spine
Abstract
Background: Correct sagittal alignment with a balanced pelvis and spine is crucial in the management of spinal disorders. The pelvic incidence (PI) describes the sagittal pelvic alignment and is position-independent. It has barely been investigated on CT scans. Furthermore, no studies have focused on the association between PI and facet joint (FJ) arthritis and orientation. Therefore, our goal was to clarify the remaining issues about PI in regard to (1) physiologic values, (2) age, (3) gender, (4) lumbar lordosis (LL) and (5) FJ arthritis and orientation using CT scans.
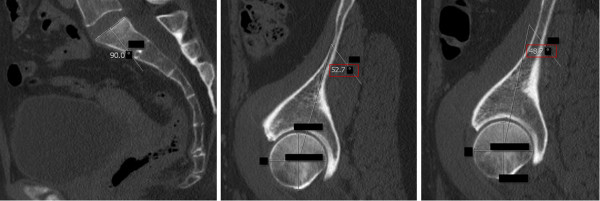
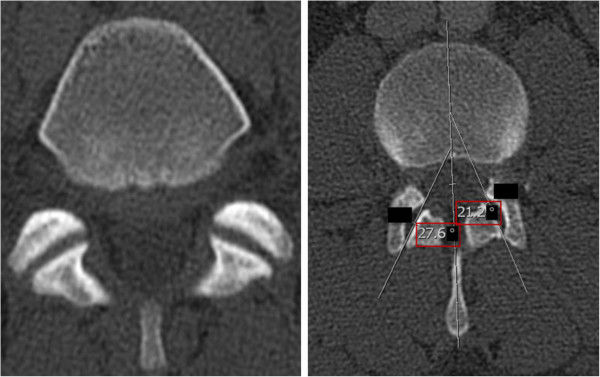
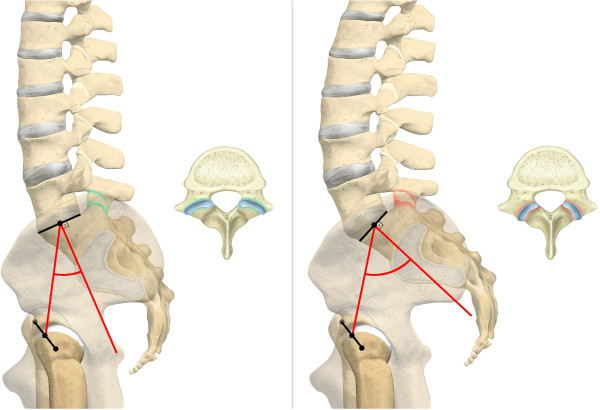
Methods: We retrospectively analyzed CT scans of 620 individuals, with a mean age of 43 years, who presented to our traumatology department and underwent a whole body CT scan, between 2008 and 2010. The PI was determined on sagittal CT planes of the pelvis by measuring the angle between the hip axis to an orthogonal line originating at the center of the superior end plate axis of the first sacral vertebra. We also evaluated LL, FJ arthritis and orientation of the lumbar spine.
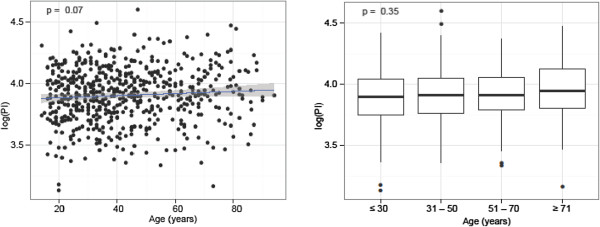
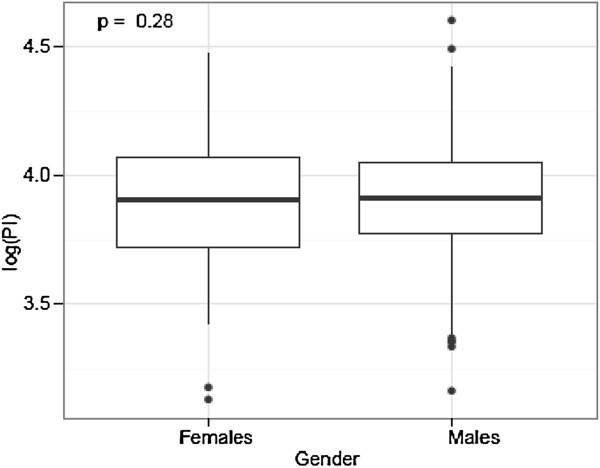
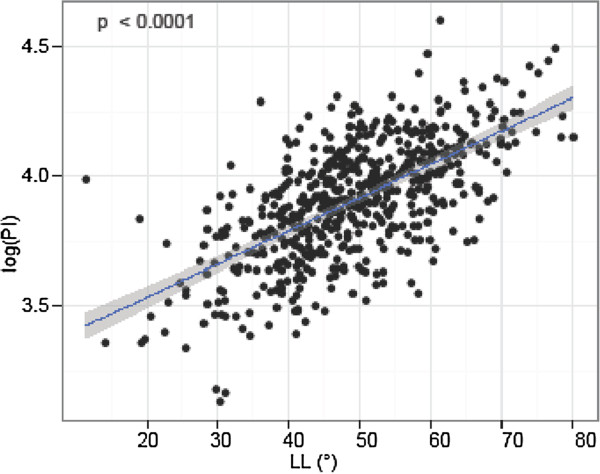
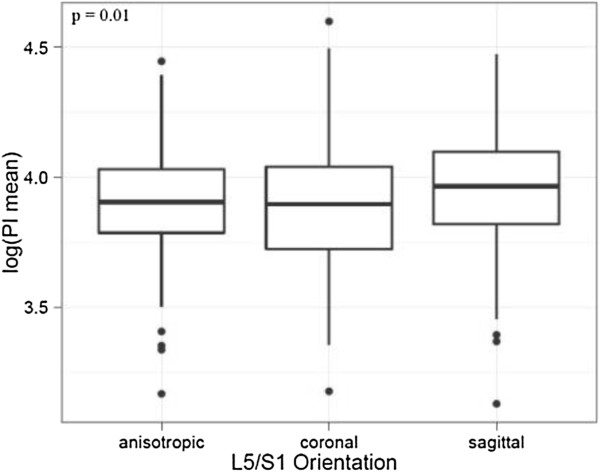
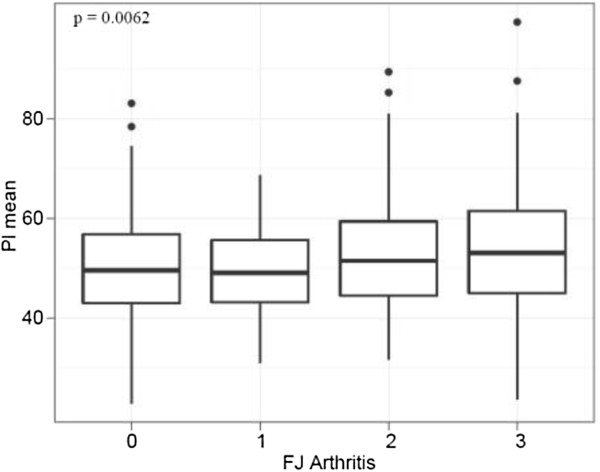
Results: 596 individuals yielded results for (1) PI with a mean of 50.8°. There was no significant difference for PI and (2) age, nor (3) gender. PI was significantly and linearly correlated with (4) LL (p = < 0.0001). Interestingly, PI and (5) FJ arthritis displayed a significant and linear correlation (p = 0.0062) with a cut-off point at 50°. An increased PI was also significantly associated with more sagitally oriented FJs at L5/S1 (p = 0.01).
Conclusion: PI is not correlated with age nor gender. However, this is the first report showing that PI is significantly and linearly associated with LL, FJ arthritis and more sagittal FJ orientation at the lower lumbar spine. This may be caused by a higher contact force on the lower lumbar FJs by an increased PI. Once symptomatic or in the event of spinal trauma, patients with increased PI and LL could benefit from corrective surgery and spondylodesis.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
