

Liraglutide efficacy and action in non-alcoholic steatohepatitis (LEAN): study protocol for a phase II multicentre, double-blinded, randomised, controlled trial
- PMID: 24189085
- PMCID: PMC3822302
- DOI: 10.1136/bmjopen-2013-003995
Liraglutide efficacy and action in non-alcoholic steatohepatitis (LEAN): study protocol for a phase II multicentre, double-blinded, randomised, controlled trial
Abstract
Introduction: Non-alcoholic steatohepatitis (NASH) is now the commonest cause of chronic liver disease. Despite this, there are no universally accepted pharmacological therapies for NASH. Liraglutide (Victoza), a human glucagon-like peptide-1 (GLP-1) analogue, has been shown to improve weight loss, glycaemic control and liver enzymes in type 2 diabetes. There is currently a lack of prospective-controlled studies investigating the efficacy of GLP-1 analogues in patients with NASH.
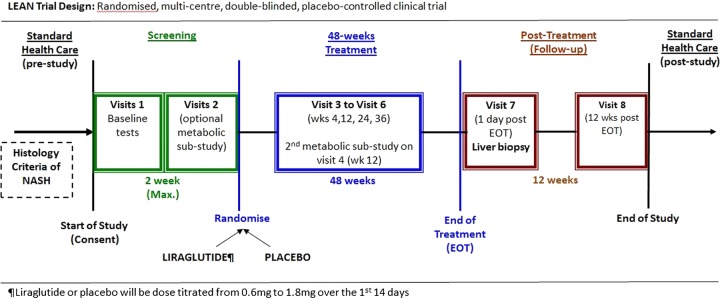
Methods and analysis: Liraglutide efficacy and action in NASH (LEAN) is a phase II, multicentre, double-blinded, placebo-controlled, randomised clinical trial designed to investigate whether a 48-week treatment with 1.8 mg liraglutide will result in improvements in liver histology in patients with NASH. Adult, overweight (body mass index ≥25 kg/m(2)) patients with biopsy-confirmed NASH were assessed for eligibility at five recruitment centres in the UK. Patients who satisfied the eligibility criteria were randomly assigned (1:1) to receive once-daily subcutaneous injections of either 1.8 mg liraglutide or liraglutide-placebo (control). Using A'Hern's single stage phase II methodology (significance level 0.05; power 0.90) and accounting for an estimated 20% withdrawal rate, a minimum of 25 patients were randomised to each treatment group. The primary outcome measure will be centrally assessed using an intention-to-treat analysis of the proportion of evaluable patients achieving an improvement in liver histology between liver biopsies at baseline and after 48 weeks of treatment. Histological improvement will be defined as a combination of the disappearance of active NASH and no worsening in fibrosis.
Ethics and dissemination: The protocol was approved by the National Research Ethics Service (East Midlands-Northampton committee; 10/H0402/32) and the Medicines and Healthcare products Regulatory Agency. Recruitment into the LEAN started in August 2010 and ended in May 2013, with 52 patients randomised. The treatment follow-up of LEAN participants is currently ongoing and is due to finish in July 2014. The findings of this trial will be disseminated through peer-reviewed publications and international presentations.
Trial registration: clinicaltrials.gov NCT01237119.
Keywords: Clinical Pharmacology; Histopathology.
Figures
References
-
- Armstrong MJ, Houlihan DD, Bentham L, et al. Presence and severity of non-alcoholic fatty liver disease in a large prospective primary care cohort. J Hepatol 2012;56:234–40 - PubMed
-
- Bellentani S, Tiribelli C, Saccoccio G, et al. Prevalence of chronic liver disease in the general population of northern Italy: the Dionysos Study. Hepatology 1994;20:1442–9 - PubMed
-
- Browning JD, Szczepaniak LS, Dobbins R, et al. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology 2004;40:1387–95 - PubMed
-
- Bellentani S, Bedogni G, Miglioli L, et al. The epidemiology of fatty liver. Eur J Gastroenterol Hepatol 2004;16:1087–93 - PubMed
-
- Williams CD, Stengel J, Asike MI, et al. Prevalence of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among a largely middle-aged population utilizing ultrasound and liver biopsy: a prospective study. Gastroenterology 2011;140:124–31 - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical