

Contemplating Alzheimer's disease and the contribution of white matter hyperintensities
- PMID: 24190781
- PMCID: PMC3874404
- DOI: 10.1007/s11910-013-0415-7
Contemplating Alzheimer's disease and the contribution of white matter hyperintensities
Abstract
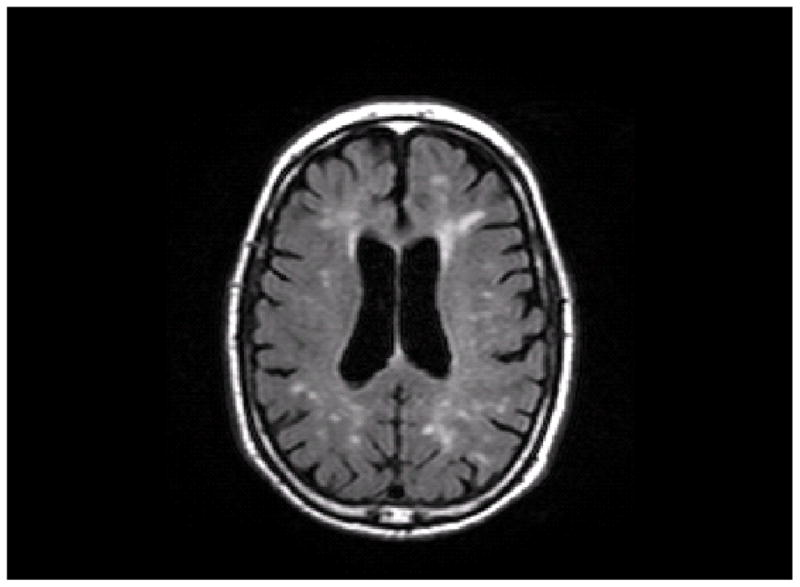
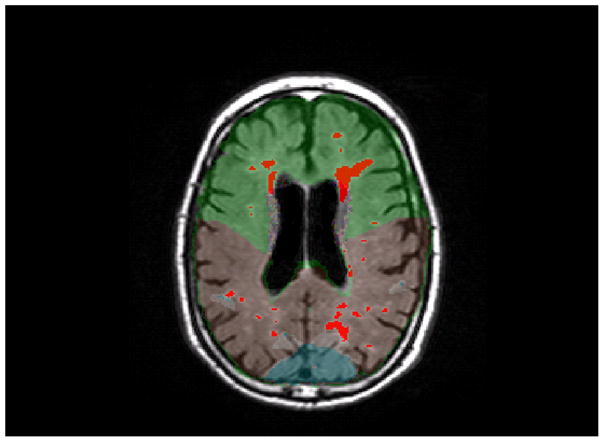
As the older adult segment of the population increases, Alzheimer's disease (AD) has emerged as a significant public health epidemic. Over the past 3 decades, advances in the understanding of the biology of AD have led to a somewhat unified hypothesis of disease pathogenesis that emphasizes the precipitating role of beta amyloid protein. However, several lines of evidence suggest that multiple pathologies are necessary for clinical manifestation of the disease. Our focus over the past several years has been on the contribution of small vessel cerebrovascular disease, visualized as white matter hyperintensities (WMH) on magnetic resonance imaging, to AD. White matter hyperintensity volume, particularly in parietal regions, is elevated among individuals with and at risk for AD, predicts future diagnosis of AD, predicts the rate of progression of cognitive symptoms among individuals with AD, and increases over time among individuals destined to develop AD. White matter hyperintensities may represent an independent source of impairment and/or may interact more fundamentally with "primary" AD pathology. Future work should focus on more inclusive models of that better define "normal" vs "pathological" aging.
Conflict of interest statement
Adam M. Brickman has received travel/accommodations expenses covered or reimbursed from the International Neuropsychological Society (as a board member) and the Alzheimer’s Association.
This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures
References
-
- Jack CR, Jr, Knopman DS, Jagust WJ, Shaw LM, Aisen PS, Weiner MW, et al. Hypothetical model of dynamic biomarkers of the Alzheimer’s pathological cascade. Lancet neurology. 2010 Jan;9(1):119–28. This paper presents a comprehensive hypothesis regarding the cascade of biological events that contribute to the pathogensis of AD. - PMC - PubMed
-
- Jack CR, Jr, Knopman DS, Jagust WJ, Petersen RC, Weiner MW, Aisen PS, et al. Tracking pathophysiological processes in Alzheimer’s disease: an updated hypothetical model of dynamic biomarkers. Lancet neurology. 2013 Feb;12(2):207–16. This paper is an updated version of a pathogenic model for Alzheimer’s disease. - PMC - PubMed
-
- Sperling RA, Aisen PS, Beckett LA, Bennett DA, Craft S, Fagan AM, et al. Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2010 May;7(3):280–92. - PMC - PubMed
-
- Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2010 May;7(3):270–9. - PMC - PubMed
-
- McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984 Jul;34(7):939–44. - PubMed
Publication types
MeSH terms
Grants and funding
- AG029949/AG/NIA NIH HHS/United States
- R01 AG034189/AG/NIA NIH HHS/United States
- R21 AG043337/AG/NIA NIH HHS/United States
- AG024708/AG/NIA NIH HHS/United States
- R56 AG034189/AG/NIA NIH HHS/United States
- AG037212/AG/NIA NIH HHS/United States
- R01 AG037212/AG/NIA NIH HHS/United States
- F32 AG024708/AG/NIA NIH HHS/United States
- K23 AG029949/AG/NIA NIH HHS/United States
- AG034189/AG/NIA NIH HHS/United States
- P01 AG007232/AG/NIA NIH HHS/United States
- R01 AG028786/AG/NIA NIH HHS/United States
- AG028786/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
