

Omega-3 PUFA supplementation and the response to evoked endotoxemia in healthy volunteers
- PMID: 24190860
- PMCID: PMC3947472
- DOI: 10.1002/mnfr.201300368
Omega-3 PUFA supplementation and the response to evoked endotoxemia in healthy volunteers
Abstract
Scope: Fish oil-derived n-3 PUFA may improve cardiometabolic health through modulation of innate immunity. However, findings in clinical studies are conflicting. We hypothesized that n-3 PUFA supplementation would dose-dependently reduce the systemic inflammatory response to experimental endotoxemia in healthy humans.
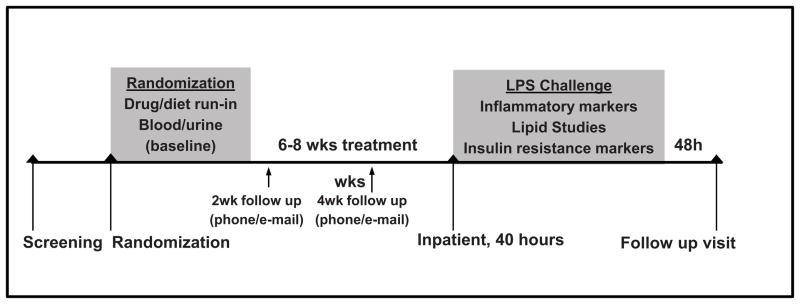
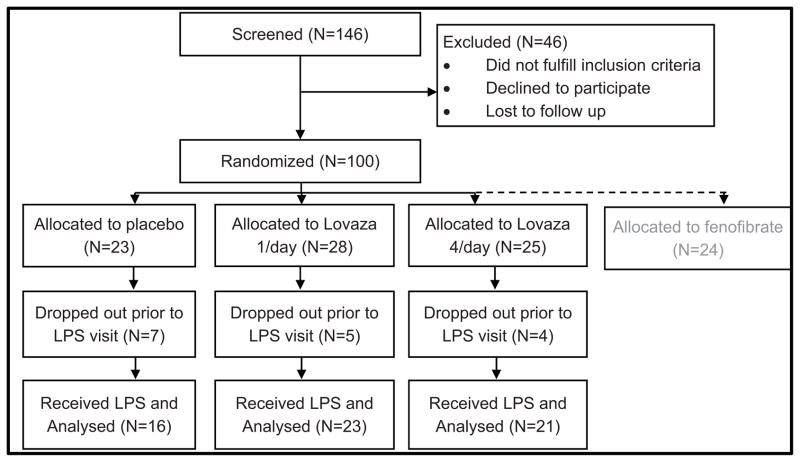
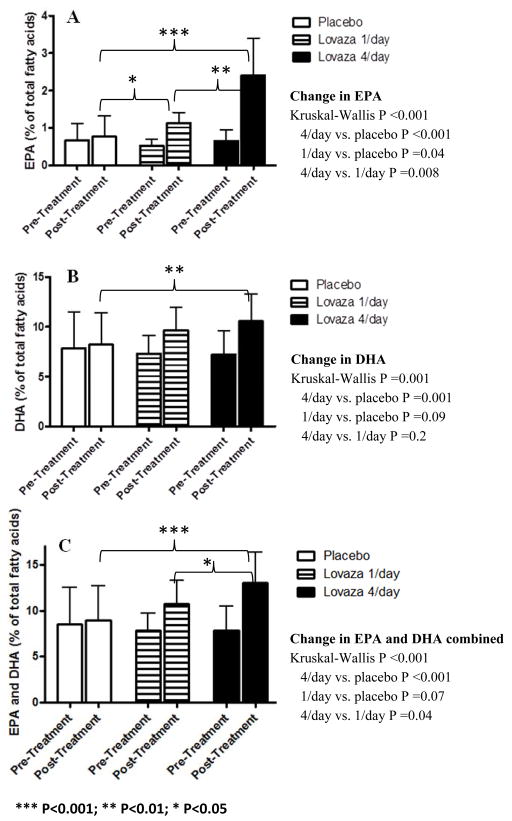
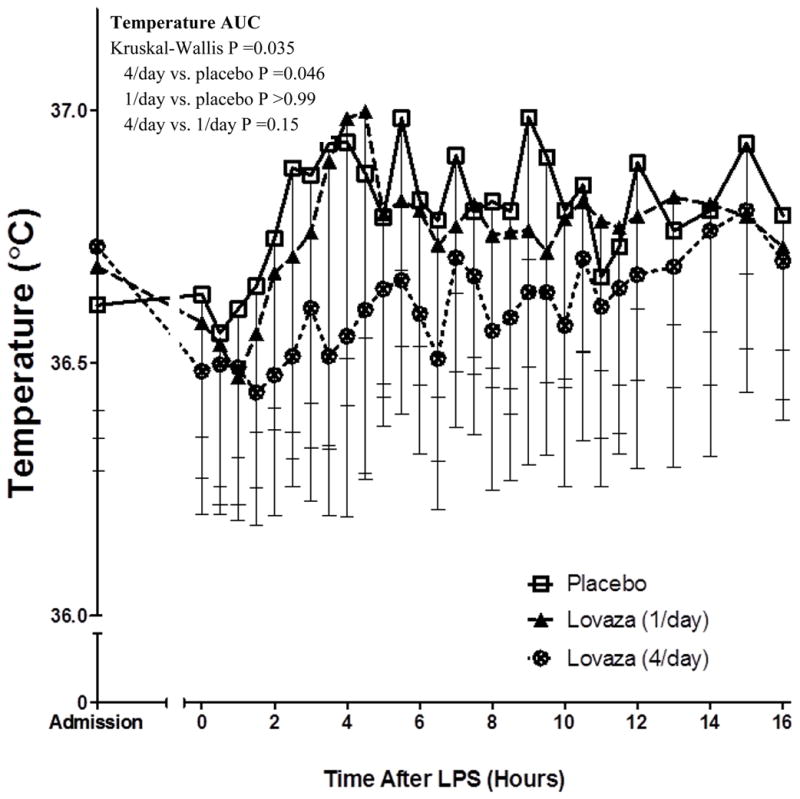
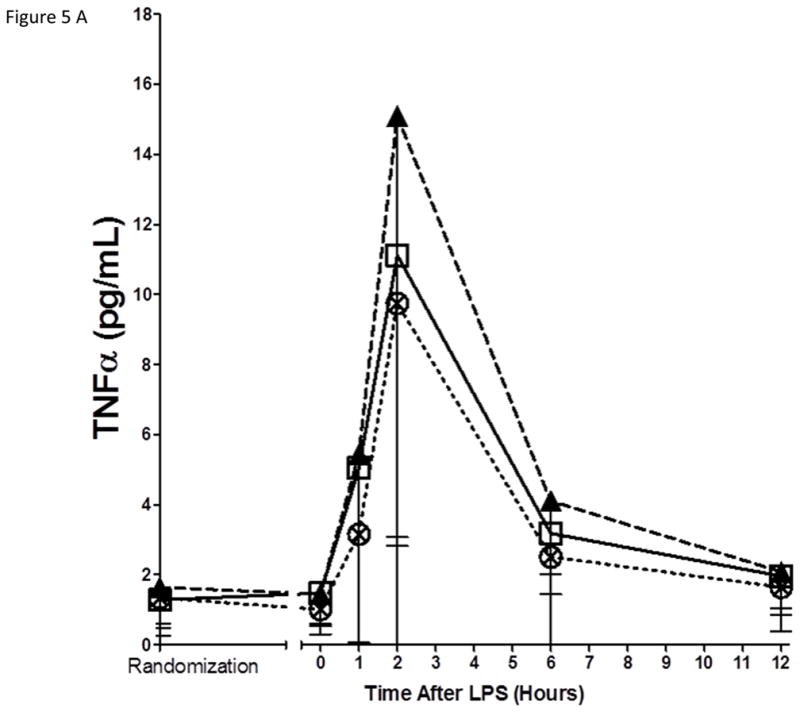
Methods and results: The Fenofibrate and omega-3 Fatty Acid Modulation of Endotoxemia (FFAME) study was an 8-wk randomized double-blind trial of placebo or n-3 PUFA supplementation (Lovaza 465 mg eicosapentaenoic acid (EPA) + 375 mg docosahexaenoic acid (DHA)) at "low" (1/day, 900 mg) or "high" (4/day, 3600 mg) dose in healthy individuals (N = 60; age 18-45; BMI 18-30; 43% female; 65% European-, 20% African-, 15% Asian-ancestry) before a low-dose endotoxin challenge (LPS 0.6 ng/kg intravenous bolus). The endotoxemia-induced temperature increase was significantly reduced with high-dose (p = 0.03) but not low-dose EPA + DHA compared to placebo. Although there was no statistically significant impact of EPA + DHA on individual inflammatory responses (tumor necrosis factor-α (TNF-α), IL-6, monocyte chemotactic protein (MCP-1), IL-1 receptor agonist (IL-1RA), IL-10, C-reactive protein (CRP), serum amyloid A (SAA)), there was a pattern of lower responses across all biomarkers with high-dose (nine of nine observed), but not low-dose EPA + DHA.
Conclusion: EPA + DHA at 3600 mg/day, but not 900 mg/day, reduced fever and had a pattern of attenuated LPS induction of plasma inflammatory markers during endotoxemia. Clinically and nutritionally relevant long-chain n-3 PUFA regimens may have specific, dose-dependent, anti-inflammatory actions.
Keywords: Endotoxemia; Fish oil; Inflammation; LPS; n-3 PUFA.
© 2013 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim.
Figures
 Lovaza (1/day) ⊗ Lovaza (4/day)
Lovaza (1/day) ⊗ Lovaza (4/day)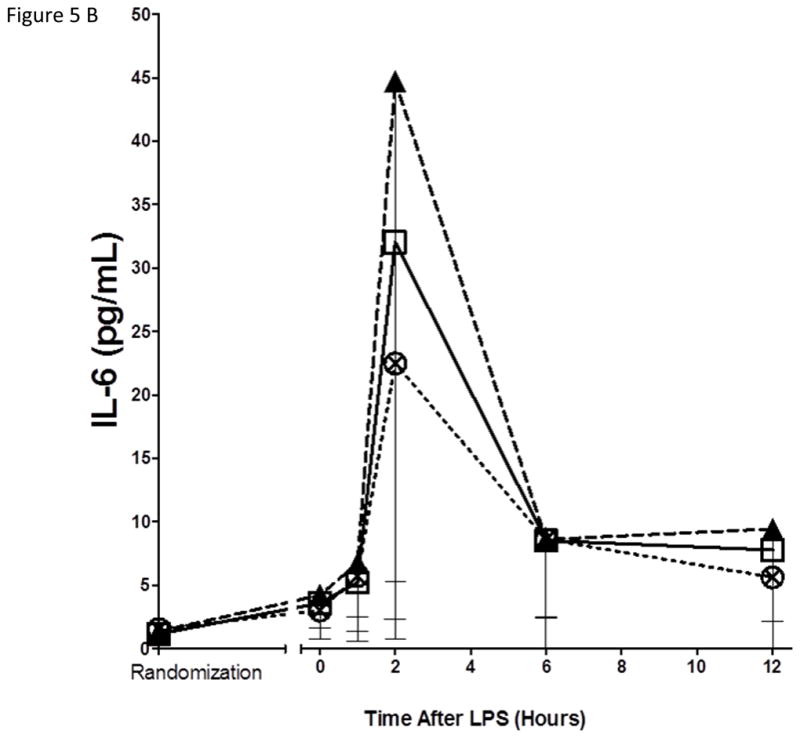 Lovaza (1/day) ⊗ Lovaza (4/day)
Lovaza (1/day) ⊗ Lovaza (4/day)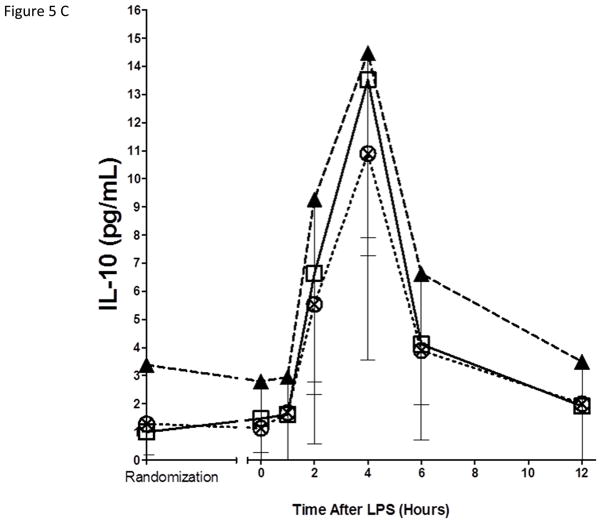 Lovaza (1/day) ⊗ Lovaza (4/day)
Lovaza (1/day) ⊗ Lovaza (4/day)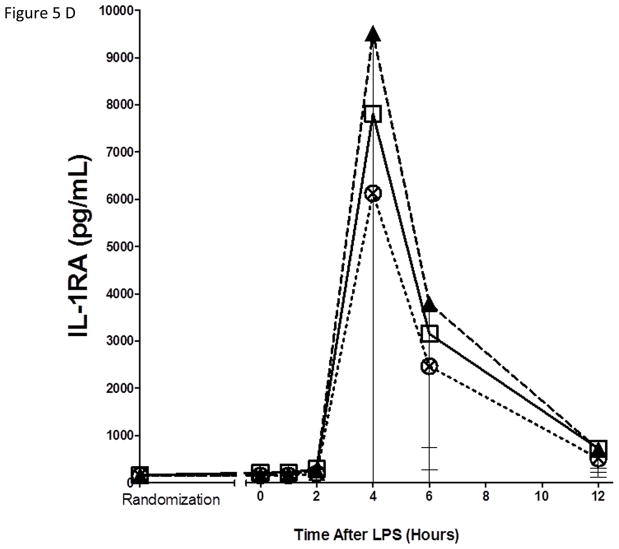 Lovaza (1/day) ⊗ Lovaza (4/day)
Lovaza (1/day) ⊗ Lovaza (4/day)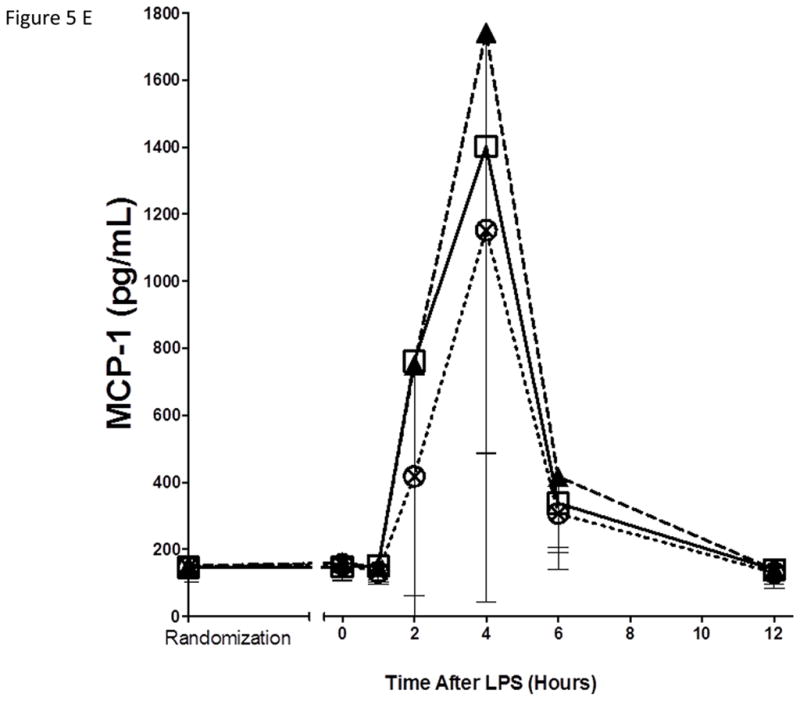 Lovaza (1/day) ⊗ Lovaza (4/day)
Lovaza (1/day) ⊗ Lovaza (4/day)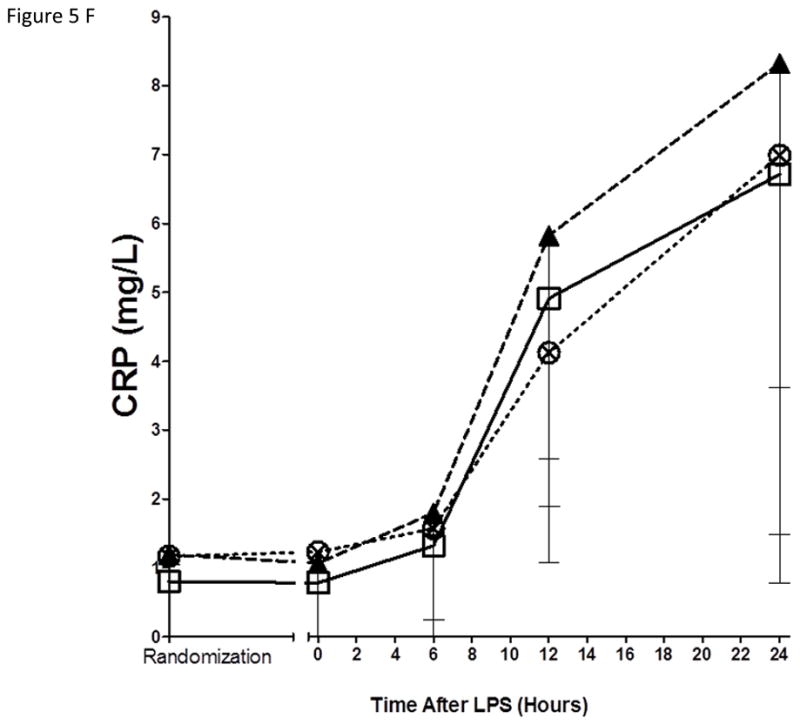 Lovaza (1/day) ⊗ Lovaza (4/day)
Lovaza (1/day) ⊗ Lovaza (4/day)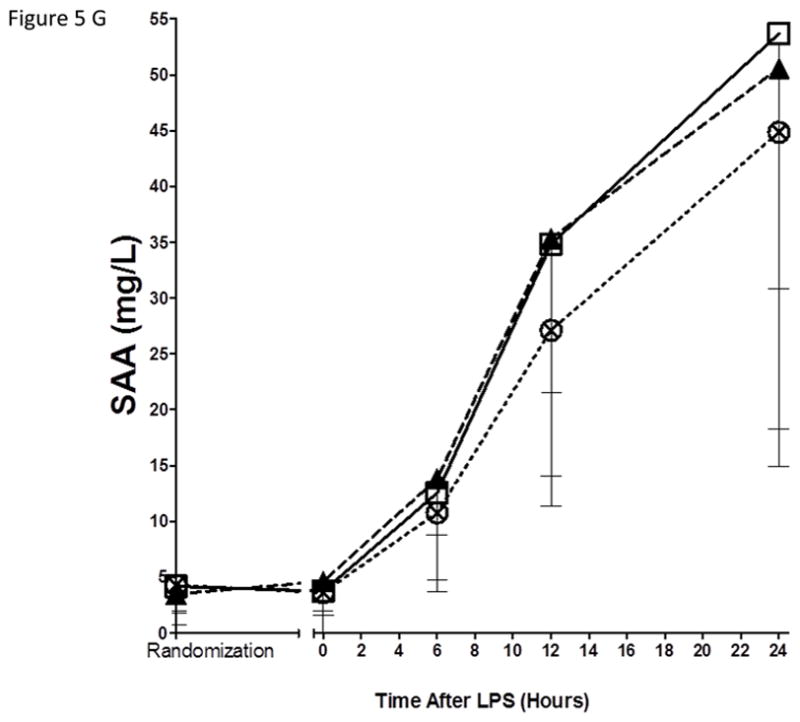 Lovaza (1/day) ⊗ Lovaza (4/day)
Lovaza (1/day) ⊗ Lovaza (4/day)References
-
- de Luca C, Olefsky JM. Stressed out about obesity and insulin resistance. Nature medicine. 2006;12:41–42. discussion 42. - PubMed
-
- Calder PC, Ahluwalia N, Brouns F, Buetler T, et al. Dietary factors and low-grade inflammation in relation to overweight and obesity. The British journal of nutrition. 2011;106(Suppl 3):S5–78. - PubMed
-
- Moreira AP, Texeira TF, Ferreira AB, do Peluzio MC, de Alfenas RC. Influence of a high-fat diet on gut microbiota, intestinal permeability and metabolic endotoxaemia. The British journal of nutrition. 2012;108:801–809. - PubMed
-
- Wang C, Harris WS, Chung M, Lichtenstein AH, et al. n-3 Fatty acids from fish or fish-oil supplements, but not alpha-linolenic acid, benefit cardiovascular disease outcomes in primary- and secondary-prevention studies: a systematic review. The American journal of clinical nutrition. 2006;84:5–17. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01-HL-111694/HL/NHLBI NIH HHS/United States
- UD99999906/MRC_/Medical Research Council/United Kingdom
- P50 HL083799/HL/NHLBI NIH HHS/United States
- R01 HL113147/HL/NHLBI NIH HHS/United States
- UO1-HL-108636/HL/NHLBI NIH HHS/United States
- P50-HL-083799/HL/NHLBI NIH HHS/United States
- R01 DK090505/DK/NIDDK NIH HHS/United States
- U01 HL108636/HL/NHLBI NIH HHS/United States
- R01 HL111694/HL/NHLBI NIH HHS/United States
- K24 HL107643/HL/NHLBI NIH HHS/United States
- MC_UP_A090_1006/MRC_/Medical Research Council/United Kingdom
- P30 DK019525/DK/NIDDK NIH HHS/United States
- R01-HL-113147/HL/NHLBI NIH HHS/United States
- R01-DK-090505/DK/NIDDK NIH HHS/United States
- K12 DK094723/DK/NIDDK NIH HHS/United States
- K23 DK095913/DK/NIDDK NIH HHS/United States
- UL1RR024134/RR/NCRR NIH HHS/United States
- K24-HL-107643/HL/NHLBI NIH HHS/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
- P20-DK 019525/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
