

Lumbar spondylolysis in juveniles from the same family: a report of three cases and a review of the literature
- PMID: 24191211
- PMCID: PMC3803119
- DOI: 10.1155/2013/272514
Lumbar spondylolysis in juveniles from the same family: a report of three cases and a review of the literature
Abstract
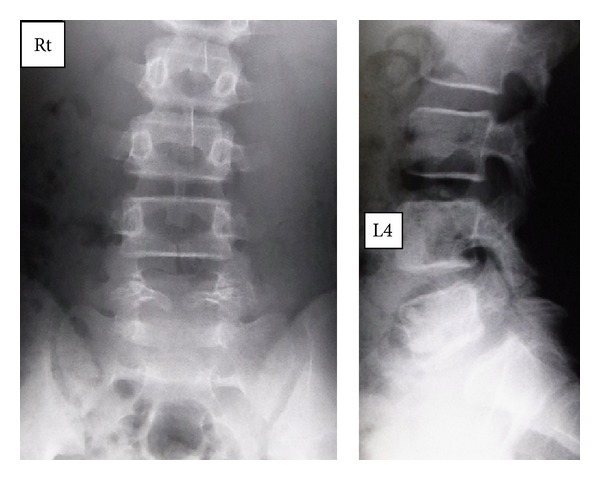
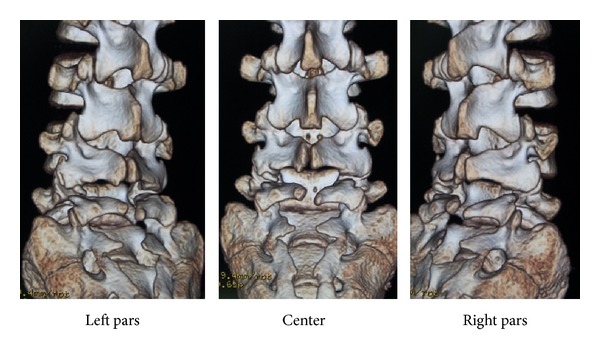
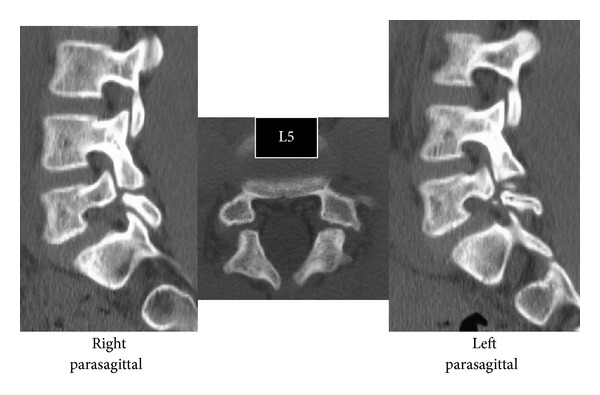
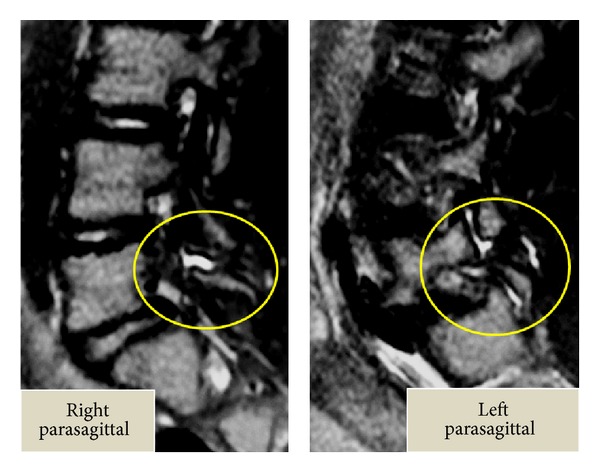
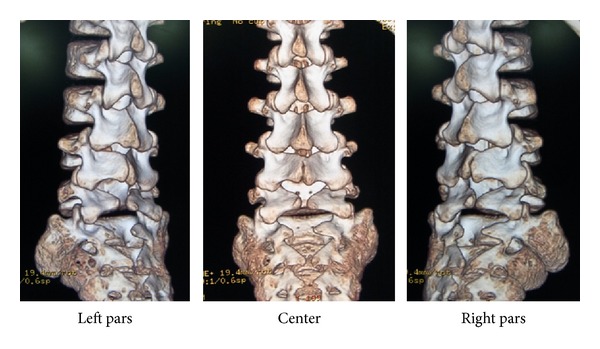
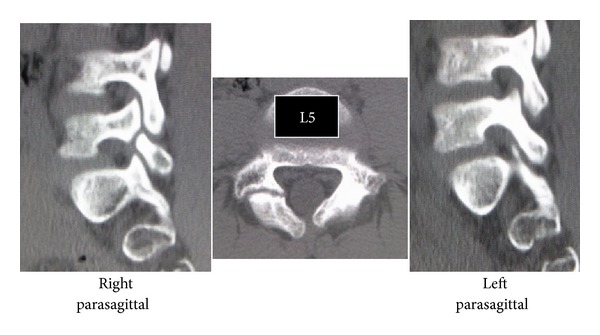
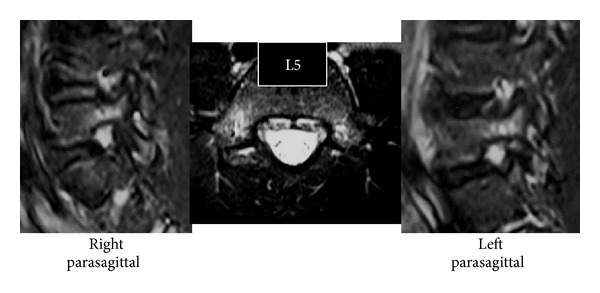
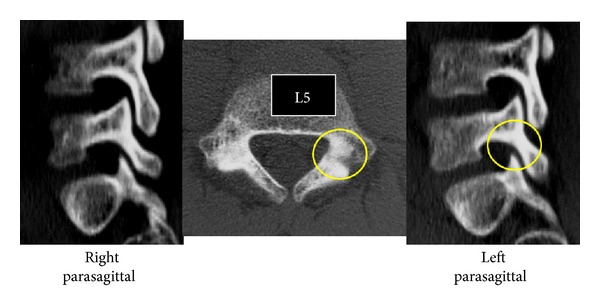
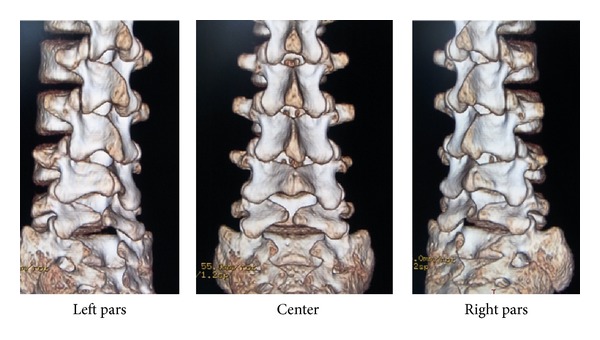
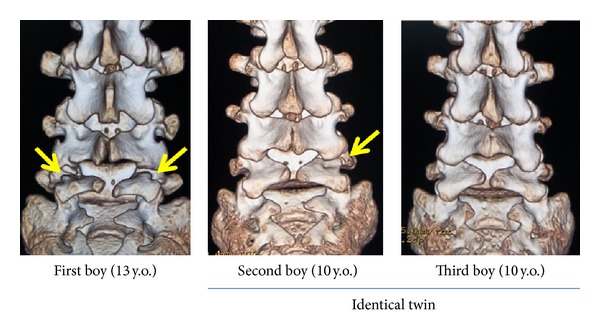
Spondylolysis is reported as a stress fracture of the pars interarticularis with a strong hereditary basis. Three cases of lumbar spondylolysis in juveniles from the same family are reported, and the genetics of the condition are reviewed. The first boy, a 13-year-old soccer player, was diagnosed with terminal stage L5 bilateral spondylolysis with grade 1 slippage. The second boy, a 10-year-old baseball player, had terminal stage right side unilateral spondylolysis. The third boy, also a 10-year-old baseball player, was diagnosed with early stage bilateral L5 spondylolysis. The second and third boys are identical twins, and all three cases exhibited concomitant spina bifida occulta. Lumbar spondylolysis has a strong hereditary basis and is reported to be an autosomal dominant condition.
Figures
References
-
- Wiltse LL. Etiology of spondylolisthesis. Clinical Orthopaedics. 1957;10:48–59. - PubMed
-
- Wiltse LL, Widell EH, Jr., Jackson DW. Fatigue fracture: the basic lesion in isthmic spondylolisthesis. The Journal of Bone & Joint Surgery A. 1975;57(1):17–22. - PubMed
-
- Wynne-Davies R, Scott JHS. Inheritance and spondylolisthesis: a radiographic family survey. The Journal of Bone & Joint Surgery B. 1979;61(3):301–305. - PubMed
-
- Haukipuro K, Keränen N, Koivisto E, et al. Familial occurrence of lumbar spondylolysis and spondylolisthesis. Clinical Genetics. 1978;13(6):471–476. - PubMed
-
- Shahriaree H, Sajadi K, Rooholamini SA. A family with spondylolisthesis. The Journal of Bone & Joint Surgery A. 1979;61(8):1256–1258. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
