

Obesity and survival in operable breast cancer patients treated with adjuvant anthracyclines and taxanes according to pathological subtypes: a pooled analysis
- PMID: 24192331
- PMCID: PMC3978725
- DOI: 10.1186/bcr3572
Obesity and survival in operable breast cancer patients treated with adjuvant anthracyclines and taxanes according to pathological subtypes: a pooled analysis
Abstract
Introduction: Obesity is an unfavorable prognostic factor in breast cancer (BC) patients regardless of menopausal status and treatment received. However, the association between obesity and survival outcome by pathological subtype requires further clarification.
Methods: We performed a retrospective analysis including 5,683 operable BC patients enrolled in four randomized clinical trials (GEICAM/9906, GEICAM/9805, GEICAM/2003-02, and BCIRG 001) evaluating anthracyclines and taxanes as adjuvant treatments. Our primary aim was to assess the prognostic effect of body mass index (BMI) on disease recurrence, breast cancer mortality (BCM), and overall mortality (OM). A secondary aim was to detect differences of such prognostic effects by subtype.
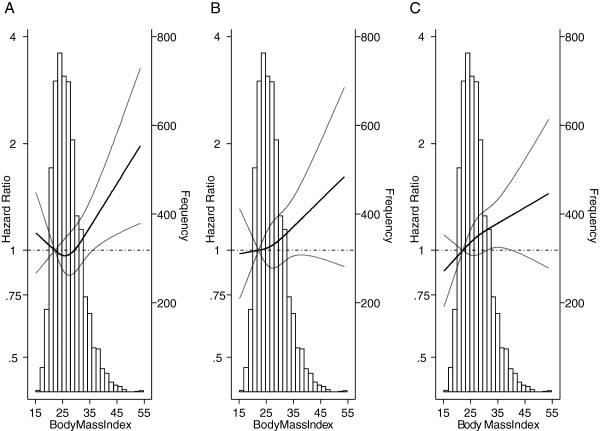
Results: Multivariate survival analyses adjusting for age, tumor size, nodal status, menopausal status, surgery type, histological grade, hormone receptor status, human epidermal growth factor receptor 2 (HER2) status, chemotherapy regimen, and under-treatment showed that obese patients (BMI 30.0 to 34.9) had similar prognoses to that of patients with a BMI < 25 (reference group) in terms of recurrence (Hazard Ratio [HR] = 1.08, 95% Confidence Interval [CI] = 0.90 to 1.30), BCM (HR = 1.02, 0.81 to 1.29), and OM (HR = 0.97, 0.78 to 1.19). Patients with severe obesity (BMI ≥ 35) had a significantly increased risk of recurrence (HR = 1.26, 1.00 to 1.59, P = 0.048), BCM (HR = 1.32, 1.00 to 1.74, P = 0.050), and OM (HR = 1.35, 1.06 to 1.71, P = 0.016) compared to our reference group. The prognostic effect of severe obesity did not vary by subtype.
Conclusions: Severely obese patients treated with anthracyclines and taxanes present a worse prognosis regarding recurrence, BCM, and OM than patients with BMI < 25. The magnitude of the harmful effect of BMI on survival-related outcomes was similar across subtypes.
Figures


References
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. GLOBOCAN 2008 v2.0, cancer incidence and mortality worldwide: iarc cancer base No. 10. Lyon, France: International Agency for Research on Cancer. 2010. [ http://globocan.iarc.fr]
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
