

Dialysis dose and intradialytic hypotension: results from the HEMO study
- PMID: 24192428
- PMCID: PMC3904183
- DOI: 10.1159/000355958
Dialysis dose and intradialytic hypotension: results from the HEMO study
Abstract
Background: Intradialytic hypotension (IDH) is common and is associated with increased morbidity and mortality in chronic hemodialysis patients. A higher dialysis 'dose' may generate transient intradialytic osmotic gradients, predisposing to intracellular fluid shifts and resulting in hypotension.
Study design: We performed a post hoc analysis of the HEMO study, a multicenter trial that randomized chronic hemodialysis patients to high versus standard Kt/V and higher versus lower membrane flux. In order to achieve dose targets, per protocol, adjustments were made in membrane efficiency, blood flow or dialysate flow before changing session length. Detailed hemodynamic and urea kinetic modeling data were abstracted from 1,825 individuals. The primary outcome was the occurrence of hypotensive events necessitating clinical intervention (saline infusion, lowering of ultrafiltration rate or reduced blood flow).
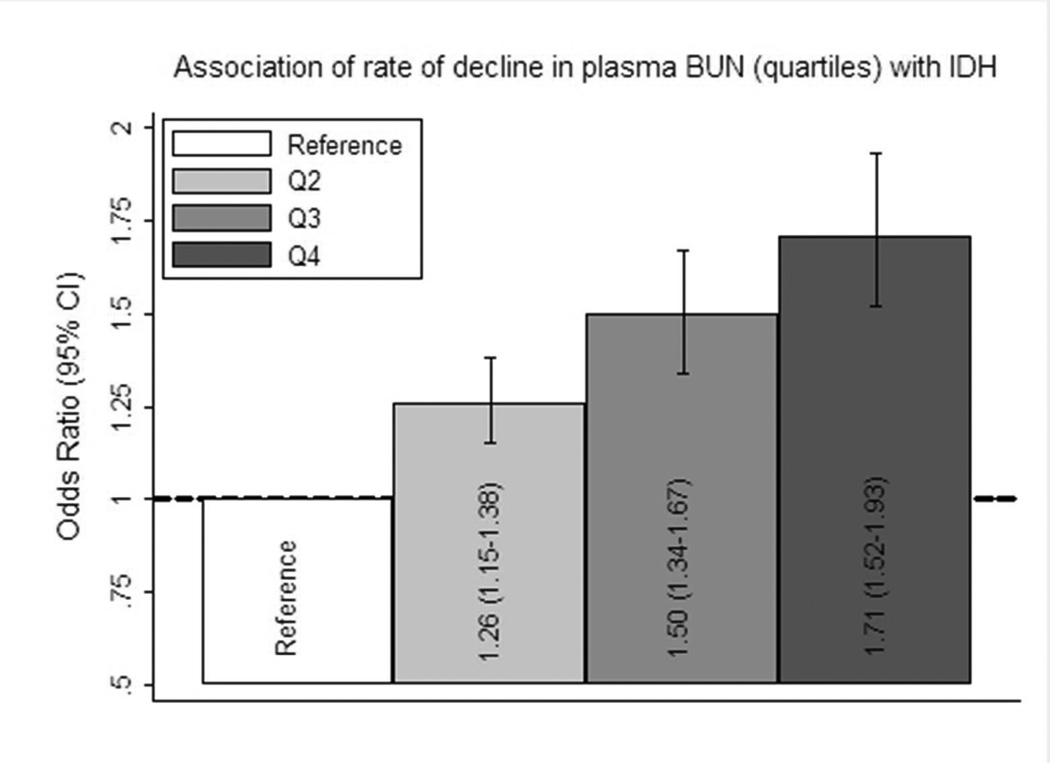
Results: Intradialytic hypotensive events occurred more frequently in the higher-Kt/V group (18.3 vs. 16.8%; p < 0.001). Participants randomized to higher-target Kt/V had a greater adjusted risk of IDH than those randomized to standard Kt/V [odds ratio (OR) 1.12; 95% confidence interval (CI) 1.01-1.25]. Higher vs. lower dialyzer mass transfer-area coefficient for urea and rate of urea removal were associated with greater adjusted odds of IDH (OR 1.15; 95% CI 1.04-1.27 and OR 1.05; 95% CI 1.04-1.06 per mg/dl/h, respectively).
Conclusions: Higher dialysis dose, at relatively constrained treatment times, may associate with an increased risk of IDH. These findings support the possibility that rapidity of intradialytic reductions in plasma osmolality may play an important role in mediating hemodynamic instability during dialysis.
© 2013 S. Karger AG, Basel.
Figures
References
-
- Bos WJ, Bruin S, van Olden RW, Keur I, Wesseling KH, Westerhof N, Krediet RT, Arisz LA. Cardiac and hemodynamic effects of hemodialysis and ultrafiltration. Am J Kidney Dis. 2000;35:819–826. - PubMed
-
- Boon D, van Montfrans GA, Koopman MG, Krediet RT, Bos WJ. Blood pressure response to uncomplicated hemodialysis: The importance of changes in stroke volume. Nephron Clin Pract. 2004;96:c82–c87. - PubMed
-
- Palmer BF, Henrich WL. Recent advances in the prevention and management of intradialytic hypotension. J Am Soc Nephrol. 2008;19:8–11. - PubMed
-
- Dheenan S, Henrich WL. Preventing dialysis hypotension: A comparison of usual protective maneuvers. Kidney Int. 2001;59:1175–1181. - PubMed
-
- KDOQI: K/doqi clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis. 2005;45:S1–S153. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
