

Gentamicin concentration gradients in scala tympani perilymph following systemic applications
- PMID: 24192668
- PMCID: PMC3918439
- DOI: 10.1159/000355283
Gentamicin concentration gradients in scala tympani perilymph following systemic applications
Abstract
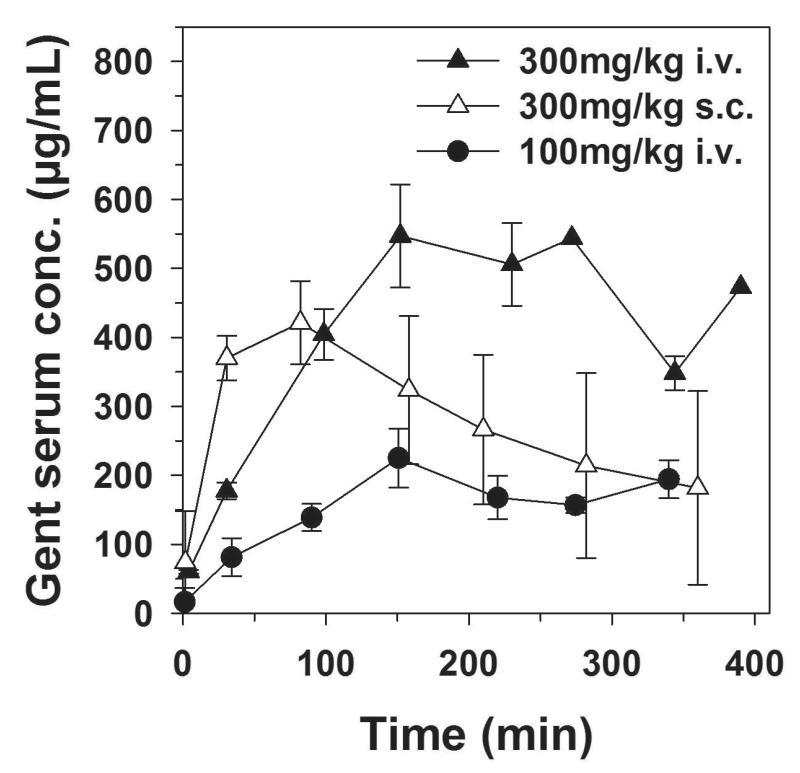
It has been shown in prior studies that round window membrane (RWM) application of gentamicin produced a robust basal-apical concentration gradient in the perilymph of scala tympani (ST) with peak concentrations in the basal turn of ST. These gradients potentially contribute to the clinical efficacy and safety of intratympanic gentamicin applications for the treatment of Ménière's disease. The present study aimed to establish the distribution of gentamicin along ST perilymph after systemic applications. Gentamicin sulfate was applied intravenously in the amounts of 100, 300 and 600 mg/kg body weight (BW) over a period of 3 h or as a 300 mg/kg BW subcutaneous bolus injection. At 3 and 5 h after the start of the application perilymph of ST was aspirated from the cochlea apex of the right and left cochlea, respectively, and 10 sequential 1-µl perilymph samples from the apex of each cochlea were quantitatively analyzed using a fluorescence polarization immunoassay. In contrast to local RWM delivery, systemic application of gentamicin resulted in the highest perilymph levels in the apex of the cochlea with decreasing concentrations towards the basal regions of ST. The absolute gentamicin concentrations increased with the amount of drug applied and time before sampling. While it is likely that the basal-apical gradient measured after local drug applications to the round window niche is the result of the direct uptake of drugs into the perilymph of the ST, distribution by diffusion and a very low perilymph flow towards the cochlear apex, computer simulations suggested that the apical-basal gradient observed with these systemic applications can be explained by higher entry rates of gentamicin in the apex compared to the basal turns of the cochlea. It is also possible that gentamicin enters perilymph indirectly from the blood via the endolymph. In this case the faster kinetics in apical turns could be due to the smaller cross-sectional area of ST relative to endolymph in the apical turns.
© 2013 S. Karger AG, Basel.
Figures





References
-
- Beck C, Schmidt CL. 10 years of experience with intratympanally applied streptomycin (gentamycin) in the therapy of Morbus Meniere. Archives of oto-rhino-laryngology. 1978;221:149–152. - PubMed
-
- Chia SH, Gamst AC, Anderson JP, Harris JP. Intratympanic gentamicin therapy for Meniere’s disease: a meta-analysis. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2004;25:544–552. - PubMed
-
- Fausti SA, Larson VD, Noffsinger D, Wilson RH, Phillips DS, Fowler CG. High-frequency audiometric monitoring strategies for early detection of ototoxicity. Ear and hearing. 1994;15:232–239. - PubMed
-
- Hoffer ME, Balough B, Henderson J, DeCicco M, Wester D, O’Leary MJ, Kopke R. Use of sustained release vehicles in the treatment of Meniere’s disease. Otolaryngol.Clin.North Am. 1997;30:1159–1166. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
