

Patient engagement programs for recognition and initial treatment of depression in primary care: a randomized trial
- PMID: 24193079
- PMCID: PMC4493759
- DOI: 10.1001/jama.2013.280038
Patient engagement programs for recognition and initial treatment of depression in primary care: a randomized trial
Abstract
Importance: Encouraging primary care patients to address depression symptoms and care with clinicians could improve outcomes but may also result in unnecessary treatment.
Objective: To determine whether a depression engagement video (DEV) or a tailored interactive multimedia computer program (IMCP) improves initial depression care compared with a control without increasing unnecessary antidepressant prescribing.
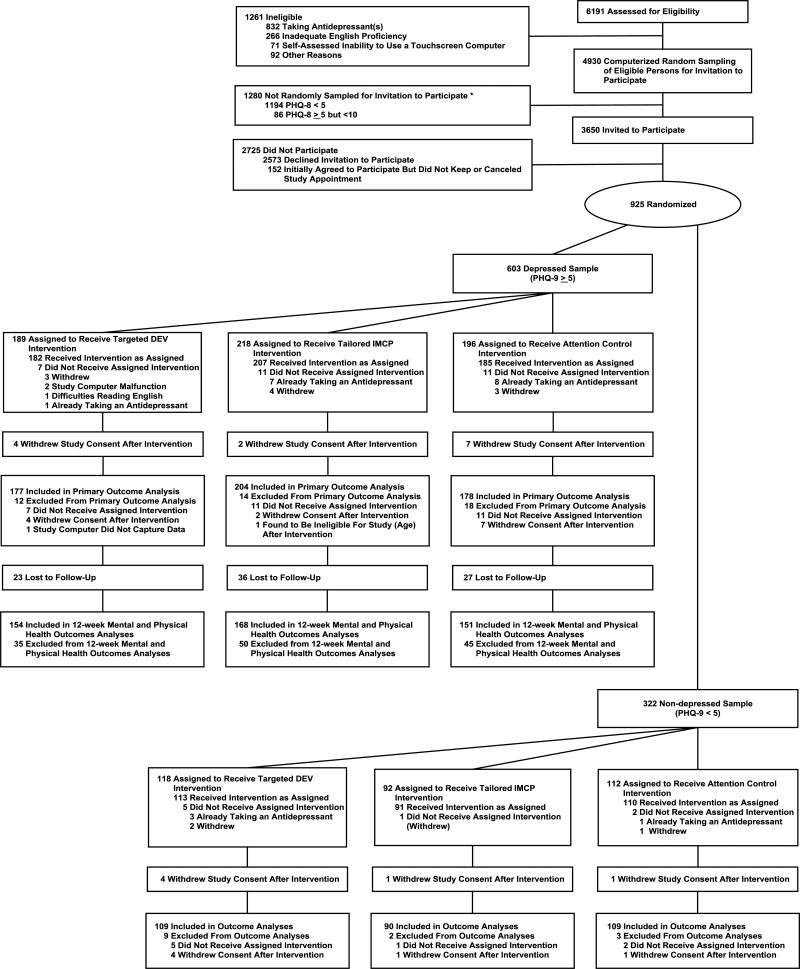
Design, setting, and participants: Randomized clinical trial comparing DEV, IMCP, and control among 925 adult patients treated by 135 primary care clinicians (603 patients with depression and 322 patients without depression, defined by Patient Health Questionnaire-9 [PHQ-9] score) conducted from June 2010 through March 2012 at 7 primary care clinical sites in California.
Interventions: DEV targeted to sex and income, an IMCP tailored to individual patient characteristics, and a sleep hygiene video (control).
Main outcomes and measures: Among depressed patients, superiority assessment of the composite measure of patient-reported antidepressant drug recommendation, mental health referral, or both (primary outcome); depression at 12-week follow-up, measured by the PHQ-8 (secondary outcome). Among nondepressed patients, noninferiority assessment of clinician- and patient-reported antidepressant drug recommendation (primary outcomes) with a noninferiority margin of 3.5%. Analyses were cluster adjusted.
Results: Of the 925 eligible patients, 867 were included in the primary analysis (depressed, 559; nondepressed, 308). Among depressed patients, rates of achieving the primary outcome were 17.5% for DEV, 26% for IMCP, and 16.3% for control (DEV vs control, 1.1 [95% CI, -6.7 to 8.9], P = .79; IMCP vs control, 9.9 [95% CI, 1.6 to 18.2], P = .02). There were no effects on PHQ-8 measured depression score at the 12-week follow-up: DEV vs control, -0.2 (95% CI, -1.2 to 0.8); IMCP vs control, 0.9 (95% CI, -0.1 to 1.9). Among nondepressed patients, clinician-reported antidepressant prescribing in the DEV and IMCP groups was noninferior to control (mean percentage point difference [PPD]: DEV vs control, -2.2 [90% CI, -8.0 to 3.49], P = .0499 for noninferiority; IMCP vs control, -3.3 [90% CI, -9.1 to 2.4], P = .02 for noninferiority); patient-reported antidepressant recommendation did not achieve noninferiority (mean PPD: DEV vs control, 0.9 [90% CI, -4.9 to 6.7], P = .23 for noninferiority; IMCP vs control, 0.3 [90% CI, -5.1 to 5.7], P = .16 for noninferiority).
Conclusions and relevance: A tailored IMCP increased clinician recommendations for antidepressant drugs, a mental health referral, or both among depressed patients but had no effect on mental health at the 12-week follow-up. The possibility that the IMCP and DEV increased patient-reported clinician recommendations for an antidepressant drug among nondepressed patients could not be excluded.
Trial registration: clinicaltrials.gov Identifier: NCT01144104.
Figures
Comment in
-
Patient engagement programs and treatment of depression.JAMA. 2014 Mar 19;311(11):1158-9. doi: 10.1001/jama.2014.576. JAMA. 2014. PMID: 24643610 No abstract available.
-
Patient engagement programs and treatment of depression--reply.JAMA. 2014 Mar 19;311(11):1159-60. doi: 10.1001/jama.2014.579. JAMA. 2014. PMID: 24643612 No abstract available.
References
-
- Berardi D, Menchetti M, Cevenini N, Scaini S, Versari M, De Ronchi D. Increased recognition of depression in primary care. Comparison between primary-care physician and ICD-10 diagnosis of depression. Psychotherapy and psychosomatics. 2005;74(4):225–230. - PubMed
-
- Lotfi L, Flyckt L, Krakau I, Martensson B, Nilsson GH. Undetected depression in primary healthcare: occurrence, severity and co-morbidity in a two-stage procedure of opportunistic screening. Nordic journal of psychiatry. 2010 Dec;64(6):421–427. - PubMed
-
- Simon GE, Fleck M, Lucas R, Bushnell DM, Group L. Prevalence and predictors of depression treatment in an international primary care study. The American journal of psychiatry. 2004 Sep;161(9):1626–1634. - PubMed
-
- Unutzer J, Katon W, Callahan CM, et al. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA : the journal of the American Medical Association. 2002 Dec 11;288(22):2836–2845. - PubMed
-
- Wells KB. Caring for depression in primary care: defining and illustrating the policy context. The Journal of clinical psychiatry. 1997;58(Suppl 1):24–27. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
