

Clinicopathological and molecular histochemical review of skull base metastasis from differentiated thyroid carcinoma
- PMID: 24194626
- PMCID: PMC3813819
- DOI: 10.1267/ahc.13019
Clinicopathological and molecular histochemical review of skull base metastasis from differentiated thyroid carcinoma
Abstract
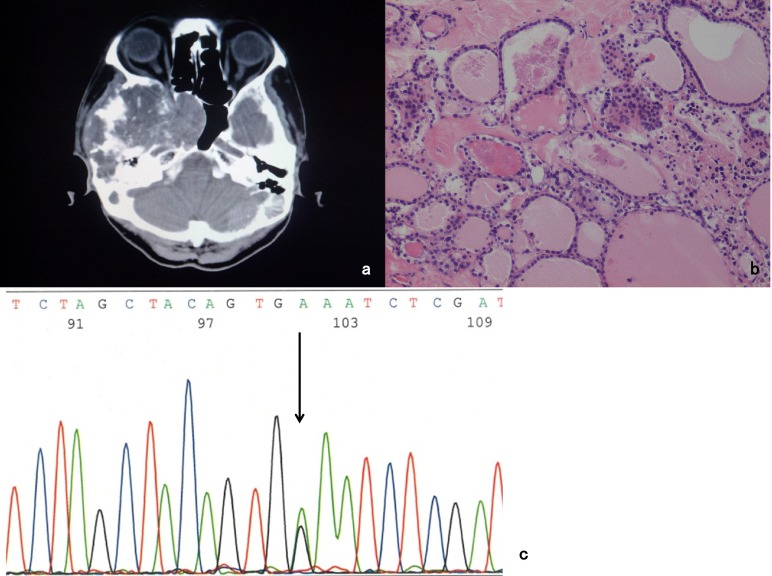
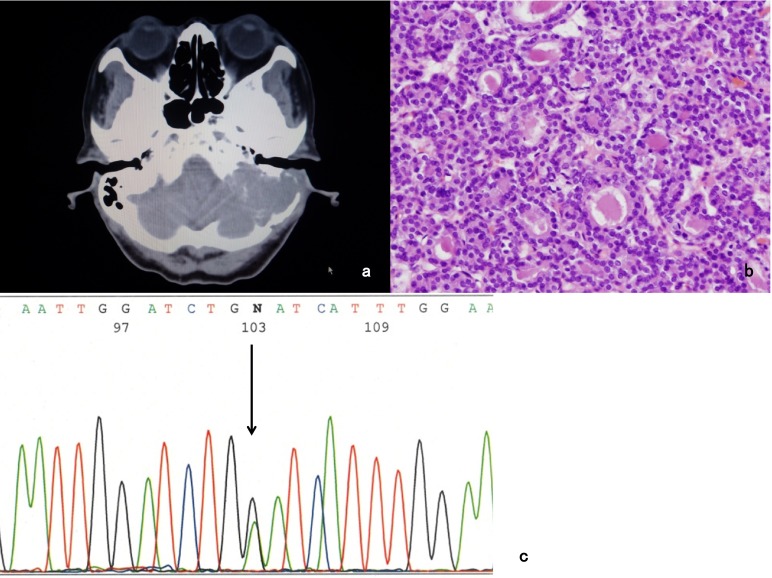
Skull base metastasis from differentiated thyroid carcinoma including follicular thyroid carcinoma (FTC) and papillary thyroid carcinoma (PTC) is a rare clinical entity. Eighteen FTC cases and 10 PTC cases showing skull base metastasis have been reported. The most common symptom of skull base metastasis from FTC and PTC is cranial nerve dysfunction. Bone destruction and local invasion to the surrounding soft tissues are common on radiological imaging. Skull base metastases can be the initial clinical presentation of FTC and PTC in the presence of silent primary sites. The possibility of skull base metastasis from FTC and PTC should be considered in patients with the clinical symptoms of cranial nerve dysfunction and radiological findings of bone destruction. A variety of genetic alterations in thyroid tumors have been identified to have a fundamental role in their tumorigenesis. Molecular histochemical studies are useful for elucidating the histopathological features of thyroid carcinoma. Recent molecular findings may provide novel molecular-based treatment strategies for thyroid carcinoma.
Keywords: follicular thyroid carcinoma; iodine-131 brachytherapy; papillary thyroid carcinoma; skull base metastasis; thyroid-stimulating hormone suppression.
Figures
Similar articles
-
Skull base metastasis from follicular thyroid carcinoma -two case reports-.Neurol Med Chir (Tokyo). 2010;50(5):421-5. doi: 10.2176/nmc.50.421. Neurol Med Chir (Tokyo). 2010. PMID: 20505304
-
Clear Cell Change in Thyroid Carcinoma: A Clinicopathologic and Molecular Study with Identification of Variable Genetic Anomalies.Thyroid. 2017 Jun;27(6):819-824. doi: 10.1089/thy.2016.0631. Epub 2017 Apr 12. Thyroid. 2017. PMID: 28293986
-
Follicular variant of papillary thyroid carcinoma is a unique clinical entity: a population-based study of 10,740 cases.Thyroid. 2013 Oct;23(10):1263-8. doi: 10.1089/thy.2012.0453. Epub 2013 Sep 11. Thyroid. 2013. PMID: 23477346 Free PMC article.
-
[Skull base metastasis from differentiated thyroid carcinoma: 3 cases report and review of literature].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2017 Jun 5;31(11):881-884. doi: 10.13201/j.issn.1001-1781.2017.11.016. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2017. PMID: 29775008 Review. Chinese.
-
Skull Metastasis Extending to the Superior Sagittal Sinus: An Unfamiliar Presentation of Papillary Thyroid Carcinoma.Cureus. 2018 Jun 5;10(6):e2738. doi: 10.7759/cureus.2738. Cureus. 2018. PMID: 30087814 Free PMC article. Review.
Cited by
-
Ultrasound-guided core needle biopsy combined with immunohistochemistry and molecular testing improve the diagnostic accuracy of bone metastases from follicular thyroid carcinoma, two case reports and analyses.Clin Case Rep. 2024 May 29;12(6):e8959. doi: 10.1002/ccr3.8959. eCollection 2024 Jun. Clin Case Rep. 2024. PMID: 38817707 Free PMC article.
-
Pituitary Metastasis of Thyroid Carcinoma: A Case Report.Am J Case Rep. 2018 Jul 31;19:896-902. doi: 10.12659/AJCR.909523. Am J Case Rep. 2018. PMID: 30061553 Free PMC article.
-
Metastatic Papillary Thyroid Carcinoma Presenting as Abducens Palsy Complicated by Ocular Neuromyotonia.Neuroophthalmology. 2016 Feb 22;40(2):97-101. doi: 10.3109/01658107.2015.1132742. eCollection 2016 Apr. Neuroophthalmology. 2016. PMID: 27928392 Free PMC article.
-
Decoding the past and future of distant metastasis from papillary thyroid carcinoma: a bibliometric analysis from 2004 to 2023.Front Oncol. 2024 Sep 5;14:1432879. doi: 10.3389/fonc.2024.1432879. eCollection 2024. Front Oncol. 2024. PMID: 39301546 Free PMC article.
-
Isolated Skull Metastasis of Follicular Carcinoma Thyroid in an Elderly Female: A Rare Case.J Clin Diagn Res. 2017 Apr;11(4):ED01-ED02. doi: 10.7860/JCDR/2017/21143.9500. Epub 2017 Apr 1. J Clin Diagn Res. 2017. PMID: 28571150 Free PMC article.
References
-
- Abubaker J., Jehan Z., Bavi P., Sultana M., Al-Harbi S., Ibrahim M., Al-Nuaim A., Ahmed M., Amin T., Al-Fehaily M., Al-Sanea O., Al-Dayel F., Uddin S., Al-Kuraya K. S. Clinicopathological analysis of papillary thyroid cancer with PIK3CA alterations in a Middle Eastern population. J. Clin. Endocrinol. Metab. . 2008;93:611–618. - PubMed
-
- Akdemir I., Erol F. S., Akpolat N., Ozveren M. F., Akfirat M., Yahsi S. Skull metastasis from thyroid follicular carcinoma with difficult diagnosis of the primary lesion. Neurol. Med. Chir. (Tokyo) 2005;45:205–208. - PubMed
-
- Aoki A., Kwak R. [A case of skull metastasis of malignant struma] No To Shinkei. 1972;24:1657–1660. (in Japanese with English abstract)
-
- Bell C. D., Kovacs K., Horvath E., Smythe H., Asa S. Papillary carcinoma of thyroid metastatic to the pituitary gland. Arch. Pathol. Lab. Med. 2001;125:935–938. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources