

Detection of specific chromosomal aberrations in urine using BCA-1 (oligo-CGH-array) enhances diagnostic sensitivity and predicts the aggressiveness of non-muscle-invasive bladder transitional cell carcinoma
- PMID: 24196429
- PMCID: PMC3961601
- DOI: 10.1007/s00345-013-1191-3
Detection of specific chromosomal aberrations in urine using BCA-1 (oligo-CGH-array) enhances diagnostic sensitivity and predicts the aggressiveness of non-muscle-invasive bladder transitional cell carcinoma
Abstract
Introduction: Bladder carcinoma (B-TCC) is the fifth most prevalent carcinoma in the United States (US) or Europe. In addition, B-TCC is the most expensive carcinoma per patient between diagnosis and death, because of its 50-80 % recurrence rate. B-TCC is an optimal carcinoma for which to detect DNA alterations in urine, which is easily obtainable. Chromosomal aberrations in tumors have been closely related to the carcinogenesis process.
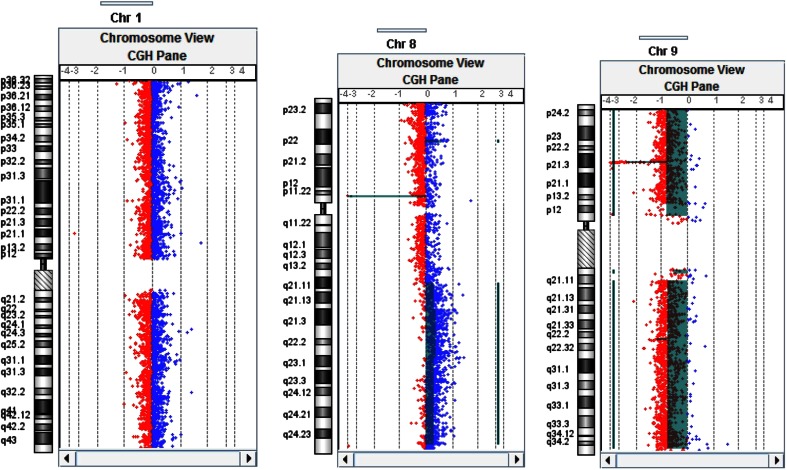
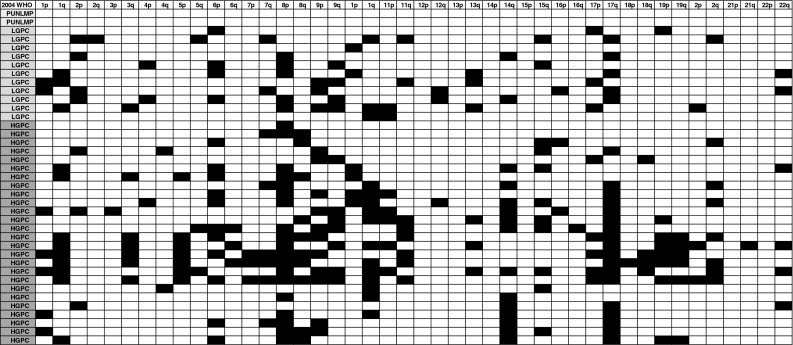
Material and methods: We developed a highly specific and sensitive oligo-CGH-array for the diagnosis and follow-up of B-TCC, based on the detection of chromosomal aberrations in urine samples. One hundred and sixty-four urine samples were analyzed. The qualitative results, including chromosomal aberrations, were obtained. Quantitative results are expressed as a percentage of chromosomal alterations on the autosomes.
Results: From the urine samples, we were able to differentiate B-TCC from non-malignant conditions with an accuracy of 100 % for patients without history of B-TCC. For follow-up of B-TCC in clinical practice, at least a deletion (8p; 9p; 9q) or a cut-off of >2 % of chromosomal imbalance was considered as a positive test. According to our criteria, 100 % of high-grade tumors were diagnosed, and the sensitivity to predict positive cystoscopy was 95 % (specificity 73 %). A cut-off >9 % was a strong signature of high-grade TCC (odds ratio 53 CI 95 % 7-417; p = 0.0002).
Conclusion: We developed a sensitive clinical tool for the detection of B-TCC using DNA extracted from patient urine. This tool is also able to identify low-grade B-TCC and identify high-risk patients harboring a high-grade disease.
Figures
References
-
- Schäfauer C, Ettori D, Rouprêt M, Phé V, Tualle JM, Tinet E, Avrillier S, Egrot C, Traxer O, Cussenot O. Detection of bladder urothelial carcinoma using in vivo noncontact, ultraviolet excited autofluorescence measurements converted into simple color coded images: a feasibility study. J Urol. 2013;190(1):271–277. doi: 10.1016/j.juro.2013.01.100. - DOI - PubMed
-
- Stenzl A, Penkoff H, Dajc-Sommerer E, Zumbraegel A, Hoeltl L, Scholz M, Riedl C, Bugelnig J, Hobisch A, Burger M, Mikuz G, Pichlmeier U. Detection and clinical outcome of urinary bladder cancer with 5-aminolevulinic acid-induced fluorescence cystoscopy : a multicenter randomized, double-blind, placebo-controlled trial. Cancer. 2011;117(5):938–947. doi: 10.1002/cncr.25523. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
