

The effect of regulatory advisories on maternal antidepressant prescribing, 1995-2007: an interrupted time series study of 228,876 pregnancies
- PMID: 24196827
- PMCID: PMC3936602
- DOI: 10.1007/s00737-013-0383-6
The effect of regulatory advisories on maternal antidepressant prescribing, 1995-2007: an interrupted time series study of 228,876 pregnancies
Abstract
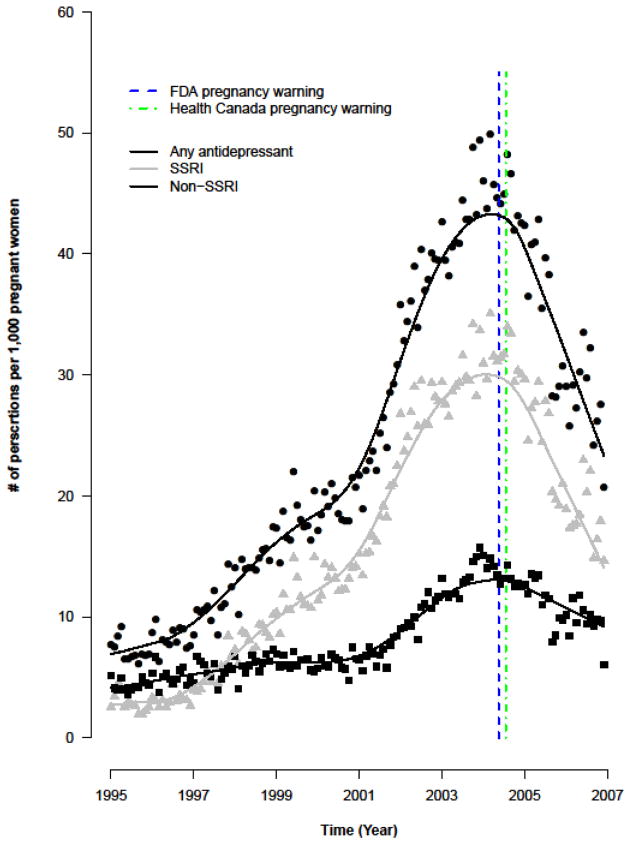
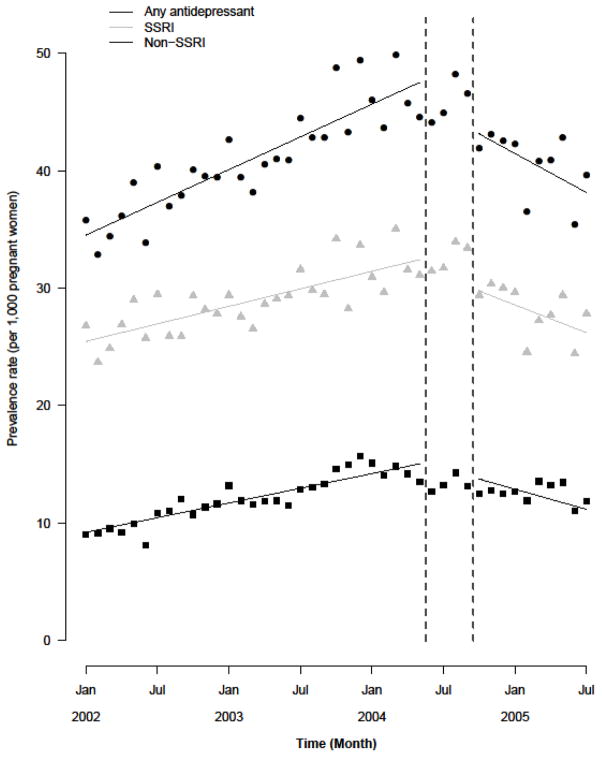
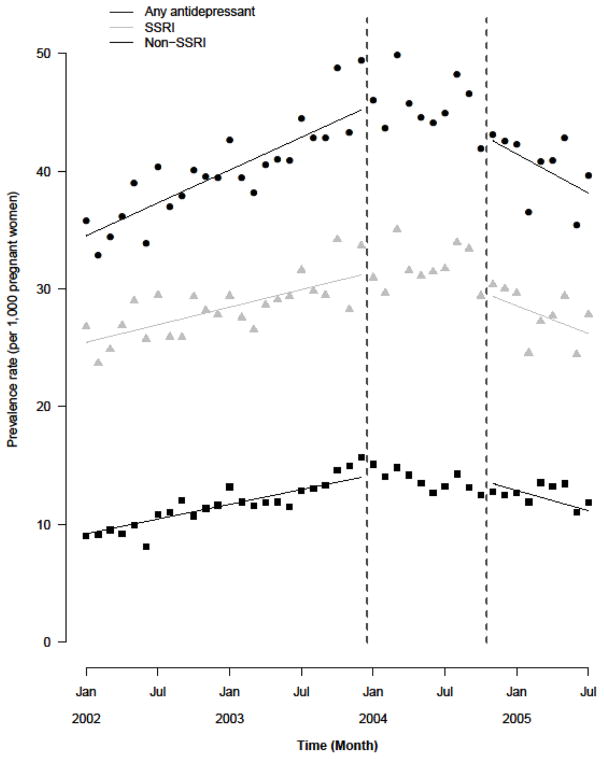
The purpose of this study was to assess whether antidepressant prescribing during pregnancy decreased following release of U.S. and Canadian public health advisory warnings about the risk of perinatal complications with antidepressants. We analyzed data from 228,876 singleton pregnancies among women (aged 15-44 years) continuously enrolled in Tennessee Medicaid with full pharmacy benefits (1995-2007). Antidepressant prescribing was determined through outpatient pharmacy dispensing files. Information on sociodemographic and clinical factors was obtained from enrollment files and linked birth certificates. An interrupted time series design with segmented regression analysis was used to quantify the impact of the advisory warnings (2002-2005). Antidepressant prescribing rates increased steadily from 1995 to 2001, followed by sharper increases from 2002 to late 2004. Overall antidepressant prescribing prevalence was 34.51 prescriptions [95 % confidence interval (CI) 33.37-35.65] per 1,000 women in January 2002, and increased at a rate of 0.46 (95 % CI 0.41-0.52) prescriptions per 1,000 women per month until the end of the pre-warning period (May 2004). During the post-warning period (October 2004-June 2005), antidepressant prescribing decreased by 1.48 (95 % CI 1.62-1.35) prescriptions per 1,000 women per month. These trends were observed for both selective serotonin reuptake inhibitors (SSRI) and non-SSRI antidepressants, although SSRI prescribing decreased at a greater rate. We conclude that antidepressant prescribing to pregnant women in Tennessee Medicaid increased from 1995 to late 2004. U.S. and Canadian public health advisories about antidepressant-associated perinatal complications were associated with steady decreases in antidepressant prescribing from late 2004 until the end of the study period, suggesting that the advisory warnings were impactful on antidepressant prescribing in pregnancy.
Figures
References
-
- Alder J, Fink N, Bitzer J, Hosli I, Holzgreve W. Depression and anxiety during pregnancy: a risk factor for obstetric, fetal and neonatal outcome? A critical review of the literature. Journal of Maternal-Fetal and Neonatal Medicine. 2007;20:189–209. - PubMed
-
- Alwan S, Reefhuis J, Rasmussen SA, Olney RS, Friedman JM. Use of selective serotonin-reuptake inhibitors in pregnancy and the risk of birth defects. N Engl J Med. 2008;356:2684–2692. - PubMed
-
- Andrade SE, Raebel MA, Brown J, Lane K, Livingston J, Boudreau D, Rolnick SJ, Roblin D, Smith DH, Willy ME, Staffa JA, Platt R. Use of antidepressant medications during pregnancy: a multisite study. Am J Obstet Gynecol. 2008;198:194–195. - PubMed
-
- Bauer M, Whybrow PC, Angst J, Versiani M, Moller HJ. World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for Biological Treatment of Unipolar Depressive Disorders, Part 1: Acute and continuation treatment of major depressive disorder. World J Biol Psychiatry. 2002;3:5–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
