

Metformin inhibits skin tumor promotion in overweight and obese mice
- PMID: 24196830
- PMCID: PMC3918668
- DOI: 10.1158/1940-6207.CAPR-13-0110
Metformin inhibits skin tumor promotion in overweight and obese mice
Abstract
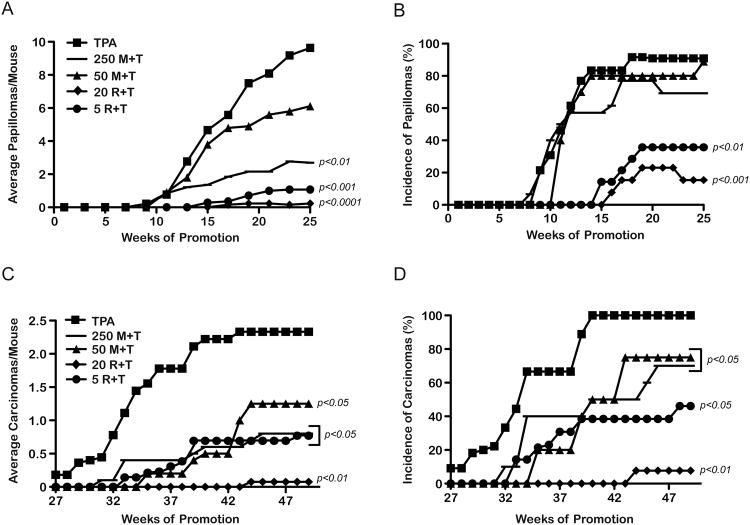
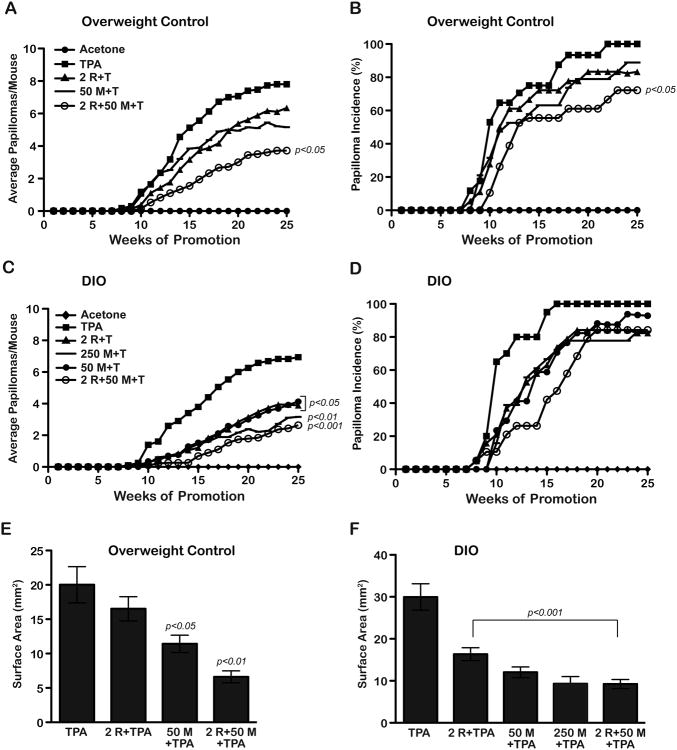
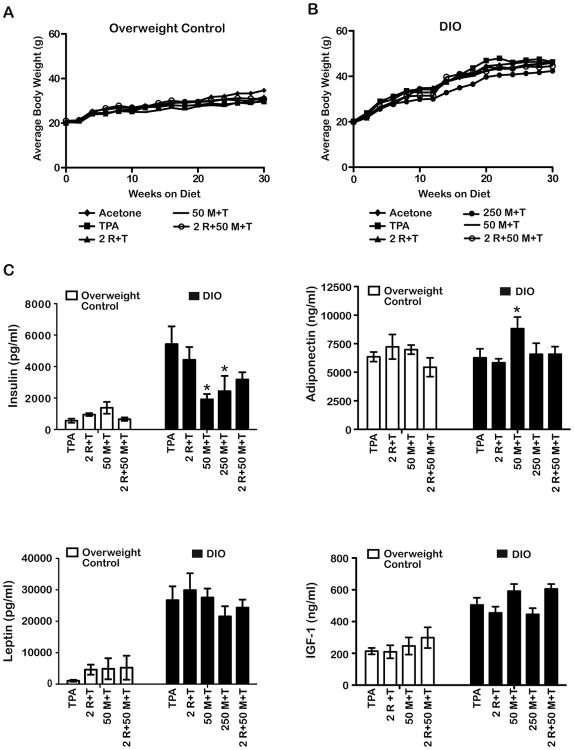
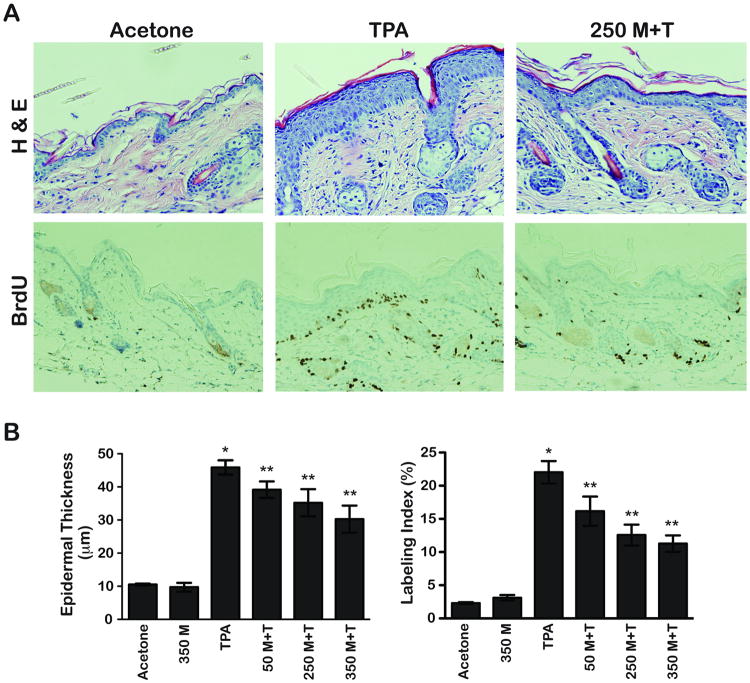
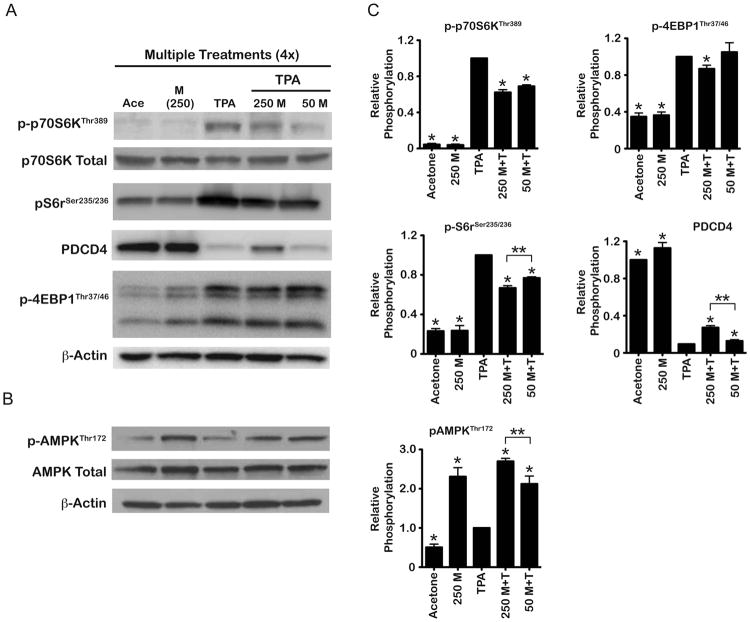
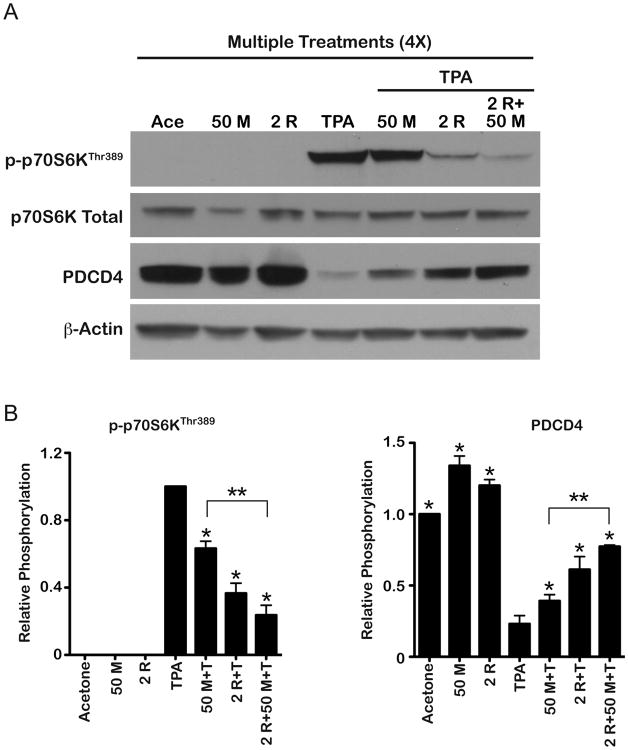
In the present study, the ability of metformin to inhibit skin tumor promotion by 12-O-tetradecanoylphorbol-13-acetate (TPA) was analyzed in mice maintained on either an overweight control diet or an obesity-inducing diet. Rapamycin was included for comparison, and a combination of metformin and rapamycin was also evaluated. Metformin (given in the drinking water) and rapamycin (given topically) inhibited development of both papillomas and squamous cell carcinomas in overweight and obese mice in a dose-dependent manner. A low-dose combination of these two compounds displayed an additive inhibitory effect on tumor development. Metformin treatment also reduced the size of papillomas. Interestingly, all treatments seemed to be at least as effective for inhibiting tumor formation in obese mice, and both metformin and rapamycin were more effective at reducing tumor size in obese mice compared with overweight control mice. The effect of metformin on skin tumor development was associated with a significant reduction in TPA-induced epidermal hyperproliferation. Furthermore, treatment with metformin led to activation of epidermal AMP-activated protein kinase (AMPK) and attenuated signaling through mTOR complex (mTORC)-1 and p70S6K. Combinations of metformin and rapamycin were more effective at blocking epidermal mTORC1 signaling induced by TPA consistent with the greater inhibitory effect on skin tumor promotion. Collectively, the current data demonstrate that metformin given in the drinking water effectively inhibited skin tumor promotion in both overweight and obese mice and that the mechanism involves activation of epidermal AMPK and attenuated signaling downstream of mTORC1.
©2013 AACR.
Figures
References
-
- Decensi A, Puntoni M, Goodwin P, Cazzaniga M, Gennari A, Bonanni B, et al. Metformin and cancer risk in diabetic patients: a systematic review and meta-analysis. Cancer Prev Res (Phila) 2010;3:1451–61. - PubMed
-
- Anisimov VN, Berstein LM, Egormin PA, Piskunova TS, Popovich IG, Zabezhinski MA, et al. Effect of metformin on life span and on the development of spontaneous mammary tumors in HER-2/neu transgenic mice. Exp Gerontol. 2005;40:685–93. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
