

Does minimally invasive transsacral fixation provide anterior column support in adult scoliosis?
- PMID: 24197391
- PMCID: PMC4016440
- DOI: 10.1007/s11999-013-3335-6
Does minimally invasive transsacral fixation provide anterior column support in adult scoliosis?
Abstract
Background: Spinal fusion to the sacrum, especially in the setting of deformity and long constructs, is associated with high complication and pseudarthrosis rates. Transsacral discectomy, fusion, and fixation is a minimally invasive spine surgery technique that provides very rigid fixation. To date, this has been minimally studied in the setting of spinal deformity correction.
Questions/purposes: We determined (1) the fusion rate of long-segment arthrodeses, (2) heath-related quality-of-life (HRQOL) outcomes (VAS pain score, Oswestry Disability Index [ODI], SF-36), and (3) the common complications and their frequency in adult patients with scoliosis undergoing transsacral fixation without supplemental pelvic fixation.
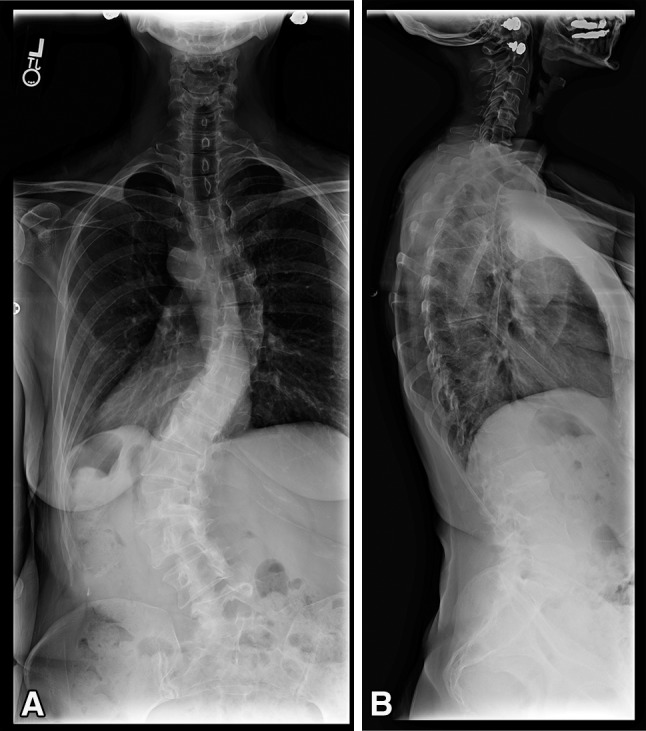
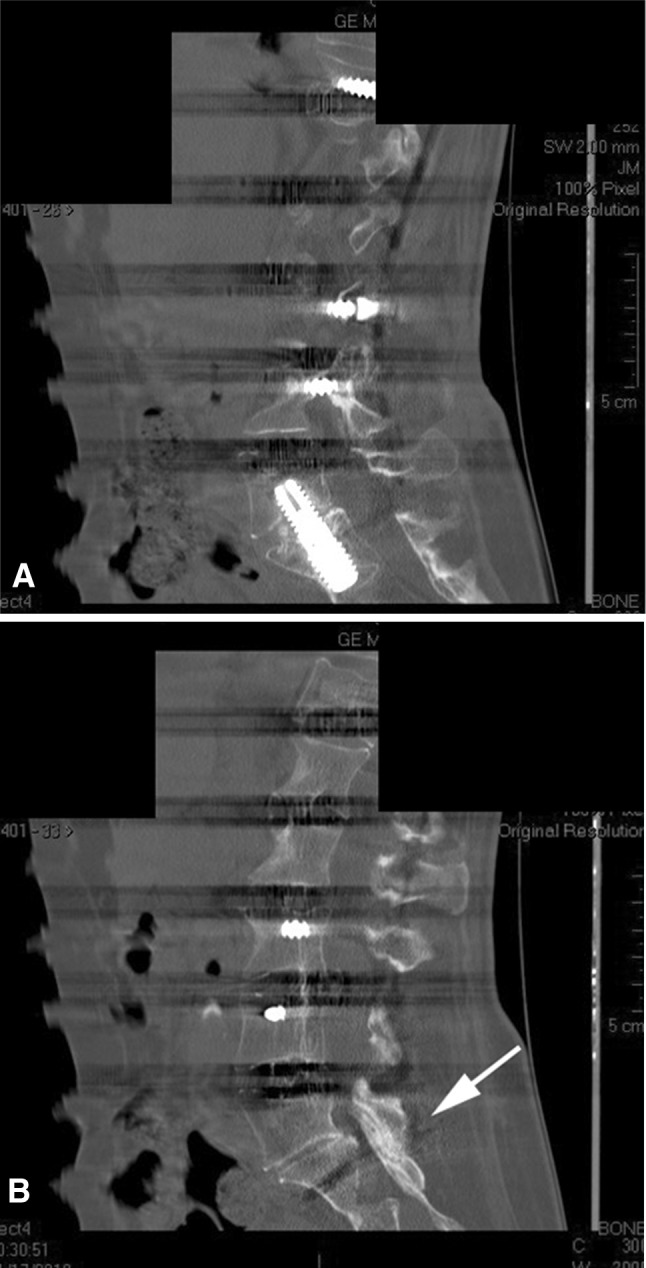
Methods: Between April 2007 and May 2011, 92 patients had fusion of three or more segments extending to the sacrum for spinal deformity. Transsacral L5-S1 fusion without supplemental pelvic fixation was performed in 56 patients. Of these, 46 with complete data points and a minimum of 2 years of followup (mean, 48 months; range, 24-72 months; 18% of patients lost to followup) were included in this study. Nineteen of the 46 (41%) had fusions extending above the thoracolumbar junction, with one patient having fusion into the proximal thoracic spine (T3-S1). General indications for the use of transsacral fixation were situations where the fusion needed to be extended to the sacrum, such as spondylolisthesis, prior laminectomy, stenosis, oblique take-off, and disc degeneration at L5-S1. Contraindications included anatomic variations in the sacrum, vascular anomalies, prior intrapelvic surgery, and rectal fistulas or abscesses. Fusion rates were assessed by full-length radiographs and CT scanning. HRQOL data, including VAS pain score, ODI, and SF-36 scores, were assessed at all pre- and postoperative visits. Intraoperative and postoperative complications were noted.
Results: Forty-one of 46 patients (89%) developed a solid fusion at L5-S1. There were significant improvements in all HRQOL parameters. Eight patients had complications related to the transsacral fusion, including five pseudarthroses and three superficial wound dehiscences. Three patients underwent revision surgery with iliac fixation. There were no bowel injuries, sacral hematomas, or sacral fractures.
Conclusions: Transsacral fixation/fusion may allow for safe lumbosacral fusion without iliac fixation in the setting of long-segment constructs in carefully selected patients. This study was retrospective and suffered from some loss to followup; future prospective trials are called for to compare this technique to other, more established approaches.
Level of evidence: Level IV, therapeutic study. See Instructions for Authors for a complete description of levels of evidence.
Figures

References
-
- Anand N, Baron EM. Presacral approaches for minimally invasive spinal fusion. In: Phillips FM, Lieberman I, Polly DW Jr, editors. Miimally Invasive Spine Surgery: Surgical Techniques & Disease Management. New York, NY: Springer; 2013.
-
- Anand N, Baron EM, Rosemann R, Hartl R, Kitchel S, Patel V. Safety and complication profile of percutaneous lumbosacral interbody fusion. Presented at Congress of Neurological Surgeons, New Orleans, LA, October 24 to 29, 2009.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
