

Ambulatory treatment of type 2 diabetes in the U.S., 1997-2012
- PMID: 24198301
- PMCID: PMC4178325
- DOI: 10.2337/dc13-2097
Ambulatory treatment of type 2 diabetes in the U.S., 1997-2012
Abstract
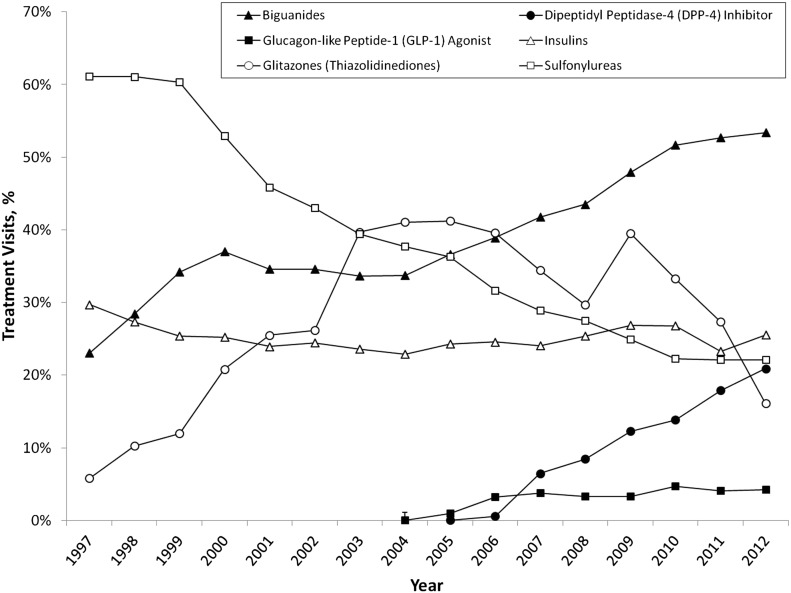
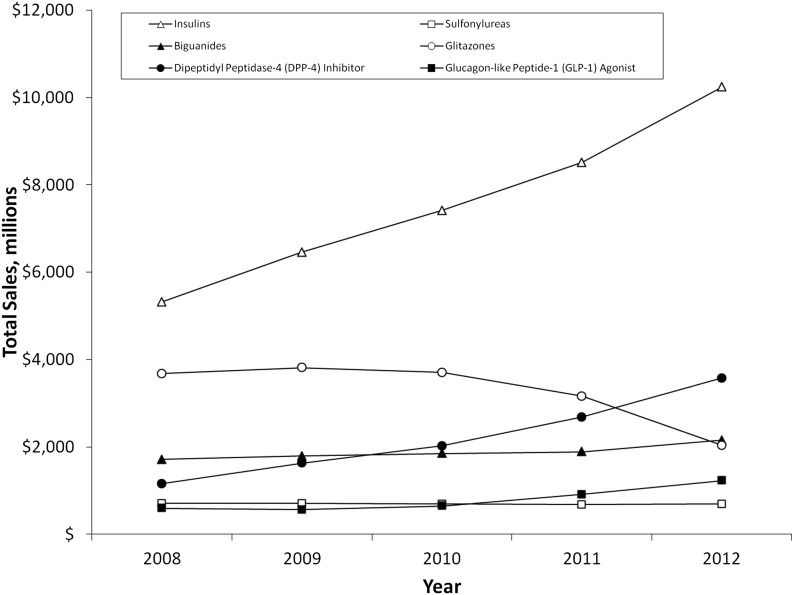
OBJECTIVE Type 2 diabetes is increasingly common and associated with substantial morbidity and mortality. This study examines trends in the patterns and costs of drug treatment of type 2 diabetes from 1997 to 2012. RESEARCH DESIGN AND METHODS We conducted descriptive analyses of cross-sectional data using the IMS Health National Disease and Therapeutic Index, a nationally representative audit of ambulatory physician practices in the U.S. We focused on visits for diabetes among patients 35 years of age or older. We used the IMS Health National Prescription Audit of pharmacy dispensing to derive information about drug expenditures. RESULTS Ambulatory diabetes visits increased from 23 million treatment visits in 1997 (95% CI 21-25) to 35 million (32-37) in 2007 and declined to 31 million visits by 2012 (27-31). Between 1997 and 2012 biguanide use increased, from 23% (20-26) to 53% (50-56) of treatment visits. Glitazone use grew from 6% (4-8) in 1997 (41% [39-43] of all visits in 2005), but declined to 16% (14-18) by 2012. Since 2005, dipeptidyl peptidase-4 (DPP-4) inhibitor use increased steadily, representing 21% (18-23) of treatment visits by 2012. Glucagon-like peptide 1 (GLP-1) agonists accounted for 4% of treatment visits in 2012. Visits where two or more drug compounds were used increased nearly 40% from 1997 to 2012. Between 2008 and 2012, drug expenditures increased 61%, driven primarily by use of insulin glargine and DPP-4 inhibitors. CONCLUSIONS Declining sulfonylurea and glitazone use has been offset by increases in DPP-4 inhibitor use and, to a lesser degree, use of GLP-1 agonists. Treatment of diabetes has grown in complexity while older treatments continue to be replaced or supplemented by newer therapies.
Figures
Similar articles
-
Ambulatory noninsulin treatment of type 2 diabetes mellitus in the United States, 2015 to 2019.Diabetes Obes Metab. 2021 Aug;23(8):1843-1850. doi: 10.1111/dom.14408. Epub 2021 May 6. Diabetes Obes Metab. 2021. PMID: 33881795
-
Trends in Insulin Types and Devices Used by Adults With Type 2 Diabetes in the United States, 2016 to 2020.JAMA Netw Open. 2021 Oct 1;4(10):e2128782. doi: 10.1001/jamanetworkopen.2021.28782. JAMA Netw Open. 2021. PMID: 34636912 Free PMC article.
-
Sulfonylurea Prescribing Patterns After the Introduction of DPP-4 Inhibitors and GLP-1 Receptor Agonists.Clin Ther. 2015 Jul 1;37(7):1477-1482.e1. doi: 10.1016/j.clinthera.2015.04.011. Epub 2015 May 27. Clin Ther. 2015. PMID: 26024569
-
Cardiovascular Actions and Clinical Outcomes With Glucagon-Like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors.Circulation. 2017 Aug 29;136(9):849-870. doi: 10.1161/CIRCULATIONAHA.117.028136. Circulation. 2017. PMID: 28847797 Review.
-
GLP-1 agonists and dipeptidyl-peptidase IV inhibitors.Handb Exp Pharmacol. 2011;(203):53-74. doi: 10.1007/978-3-642-17214-4_3. Handb Exp Pharmacol. 2011. PMID: 21484567 Review.
Cited by
-
Association of Initiation of Basal Insulin Analogs vs Neutral Protamine Hagedorn Insulin With Hypoglycemia-Related Emergency Department Visits or Hospital Admissions and With Glycemic Control in Patients With Type 2 Diabetes.JAMA. 2018 Jul 3;320(1):53-62. doi: 10.1001/jama.2018.7993. JAMA. 2018. PMID: 29936529 Free PMC article.
-
The Infamous, Famous Sulfonylureas and Cardiovascular Safety: Much Ado About Nothing?Curr Diab Rep. 2017 Oct 23;17(12):124. doi: 10.1007/s11892-017-0954-4. Curr Diab Rep. 2017. PMID: 29063276 Review.
-
Individualized Glycemic Control for U.S. Adults With Type 2 Diabetes: A Cost-Effectiveness Analysis.Ann Intern Med. 2018 Feb 6;168(3):170-178. doi: 10.7326/M17-0537. Epub 2017 Dec 12. Ann Intern Med. 2018. PMID: 29230472 Free PMC article.
-
Changes in Antidiabetic Drug Prescription and Glycemic Control Trends in Elderly Patients with Type 2 Diabetes Mellitus from 2005-2013: An Analysis of the National Center Diabetes Database (NCDD-03).Intern Med. 2018 May 1;57(9):1229-1240. doi: 10.2169/internalmedicine.9481-17. Epub 2017 Dec 27. Intern Med. 2018. PMID: 29279487 Free PMC article.
-
Clinical assessment of hepatic de novo lipogenesis in non-alcoholic fatty liver disease.Lipids Health Dis. 2016 Sep 17;15(1):159. doi: 10.1186/s12944-016-0321-5. Lipids Health Dis. 2016. PMID: 27640119 Free PMC article. Review.
References
-
- Diabetes Statistics. Data from the 2011 National Diabetes Fact Sheet (released January 26, 2011). Available from http://www.diabetes.org/diabetes-basics/diabetes-statistics/ Accessed 22 August 2013
-
- Williams R, Van Gaal L, Lucioni C, CODE-2 Advisory Board Assessing the impact of complications on the costs of type II diabetes. Diabetologia 2002;45:S13–S17 - PubMed
-
- Alexander GC, Tseng CW. Six strategies to identify and assist patients burdened by out-of-pocket prescription costs. Cleve Clin J Med 2004;71:433–437 - PubMed
-
- Grant RW, Pirraglia PA, Meigs JB, Singer DE. Trends in complexity of diabetes care in the United States from 1991 to 2000. Arch Intern Med 2004;164:1134–1139 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
