Recorded lower esophageal pressures as a function of electronic sleeve placement and location of gastric pressure measurement in patients with hiatal hernia
- PMID: 24199008
- PMCID: PMC3816182
- DOI: 10.5056/jnm.2013.19.4.479
Recorded lower esophageal pressures as a function of electronic sleeve placement and location of gastric pressure measurement in patients with hiatal hernia
Abstract
Background/aims: In high-resolution manometry lower esophageal sphincter pressure (LESP) is measured relative to intragastric pressure, however Gastric Marker™ (GM) location used to determine resting LESP is not well established with hiatal hernia (HH). We test the hypothesis that measured resting LESP varies with HH based on GM location.
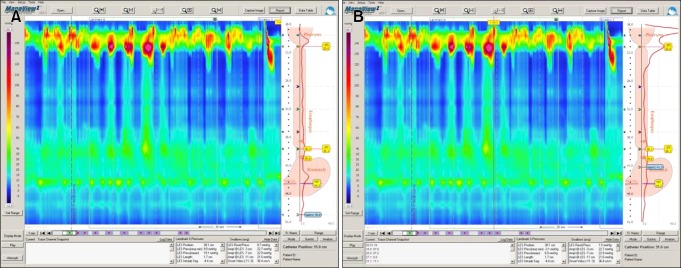
Methods: Subjects with HH ≥ 2 cm were included. The eSleeve™ was adjusted to span only the LES, excluding the crural diaphragm (CD). Resting LESP was determined by placing the GM below and above the CD (in the position yielding the highest resting LESP). Resting pressure across the lower esophageal sphincter (LES) to CD and pressure in the HH relative to subdiaphragmatic intragastric pressure were also measured.
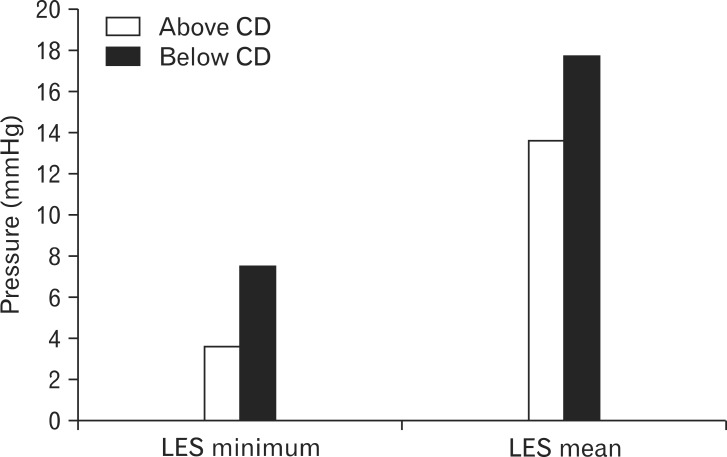
Results: HH ≥ 2 cm was present in 98 patients (mean length 2.7 cm). LESP decreased when GM was moved from below the CD into the HH: respiratory minimum LESP 7.5 ± 1.1 to 3.6 ± 0.9 mmHg; P < 0.001, mean LESP 17.7 ± 1.3 to 13.7 ± 1.1 mmHg; P < 0.001. When the eSleeve encompassed the LES and CD, the respiratory minimum pressure was 12.2 ± 0.9 mmHg and mean pressure was 23.9 ± 1.0 mmHg pressure (P < 0.001 for both). Pressure in the hernia pouch was greater than intragastric pressure: respiratory minimum 3.0 ± 0.7 mmHg and mean 9.0 ± 0.8 mmHg (P < 0.001 for both). pH studies showed a trend toward an association between abnormal distal esophagus acid exposure and lower resting LESP.
Conclusions: GM placement in the HH produces lower resting LESPs. This may provide a more physiologic representation of LESP in HH.
Keywords: Catheters; Esophagus; Gastroesophageal reflux; Hernia, hiatal; Manometry.
Conflict of interest statement
Conflicts of interest: None.
Figures
Similar articles
-
Short-term electrical stimulation of the lower esophageal sphincter increases sphincter pressure in patients with gastroesophageal reflux disease.Neurogastroenterol Motil. 2012 May;24(5):446-50, e213. doi: 10.1111/j.1365-2982.2012.01878.x. Epub 2012 Jan 31. Neurogastroenterol Motil. 2012. PMID: 22292889
-
Bolus retention in hiatal hernia identified by high-resolution esophageal manometry with impedance.Neurogastroenterol Motil. 2014 May;26(5):679-84. doi: 10.1111/nmo.12312. Epub 2014 Jan 26. Neurogastroenterol Motil. 2014. PMID: 24460884
-
[Function research of esophageal lower sphincter in infant with hiatal hernia].Zhonghua Wai Ke Za Zhi. 1999 Feb;37(2):77-9. Zhonghua Wai Ke Za Zhi. 1999. PMID: 11829784 Chinese.
-
Thoracoabdominal pressure gradient and gastroesophageal reflux: insights from lung transplant candidates.Dis Esophagus. 2018 Oct 1;31(10). doi: 10.1093/dote/doy025. Dis Esophagus. 2018. PMID: 29617746
-
Role of the lower esophageal sphincter and hiatal hernia in the pathogenesis of gastroesophageal reflux disease.J Gastrointest Surg. 1999 Jul-Aug;3(4):405-10. doi: 10.1016/s1091-255x(99)80057-2. J Gastrointest Surg. 1999. PMID: 10482693
References
-
- Pandolfino JE, Kahrilas PJ American Gastroenterological Association. AGA technical review on the clinical use of esophageal manometry. Gastroenterology. 2005;128:209–224. - PubMed
-
- Fox M, Hebbard G, Janiak P, et al. High-resolution manometry predicts the success of oesophageal bolus transport and identifies clinically important abnormalities not detected by conventional manometry. Neurogastroenterol Motil. 2004;16:533–542. - PubMed
-
- Bredenoord AJ, Weusten BL, Carmagnola S, Smout AJ. Double-peaked high-pressure zone at the esophagogastric junction in controls and in patients with a hiatal hernia: a study using high-resolution manometry. Dig Dis Sci. 2004;49:1128–1135. - PubMed
-
- Pandolfino JE, Kim H, Ghosh SK, Clarke JO, Zhang Q, Kahrilas PJ. High-resolution manometry of the EGJ: an analysis of crural CD function in GERD. Am J Gastroenterol. 2007;102:1056–1063. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources