

The role of brain MRI in mitochondrial neurogastrointestinal encephalomyopathy
- PMID: 24199812
- PMCID: PMC4202835
- DOI: 10.1177/197140091302600505
The role of brain MRI in mitochondrial neurogastrointestinal encephalomyopathy
Abstract
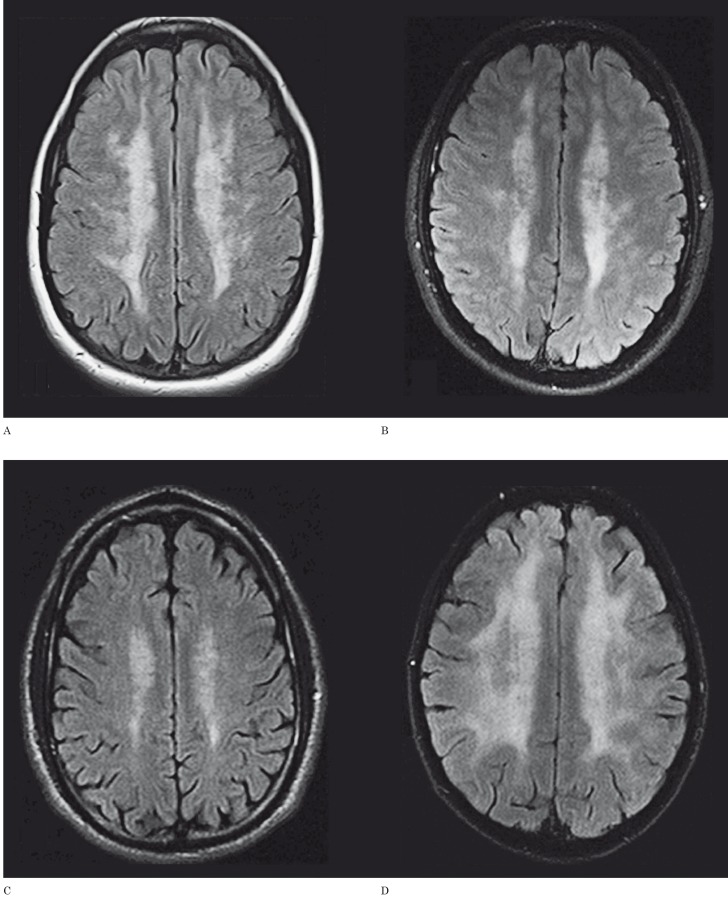
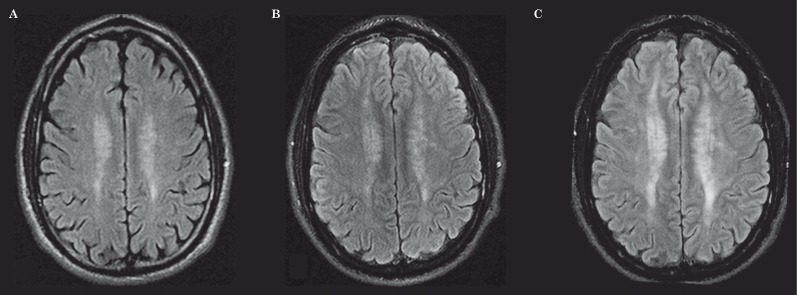
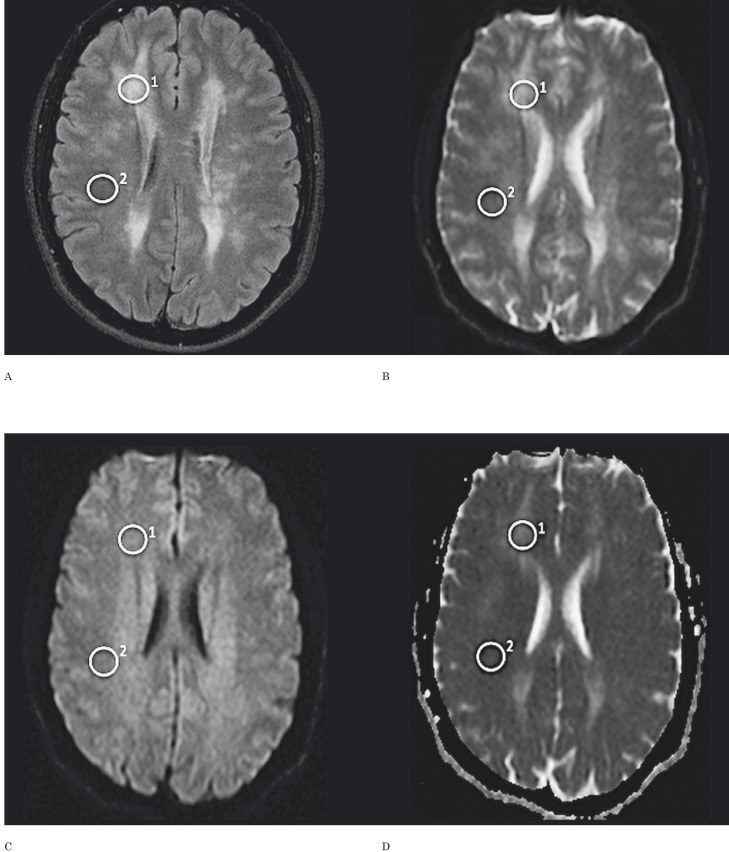
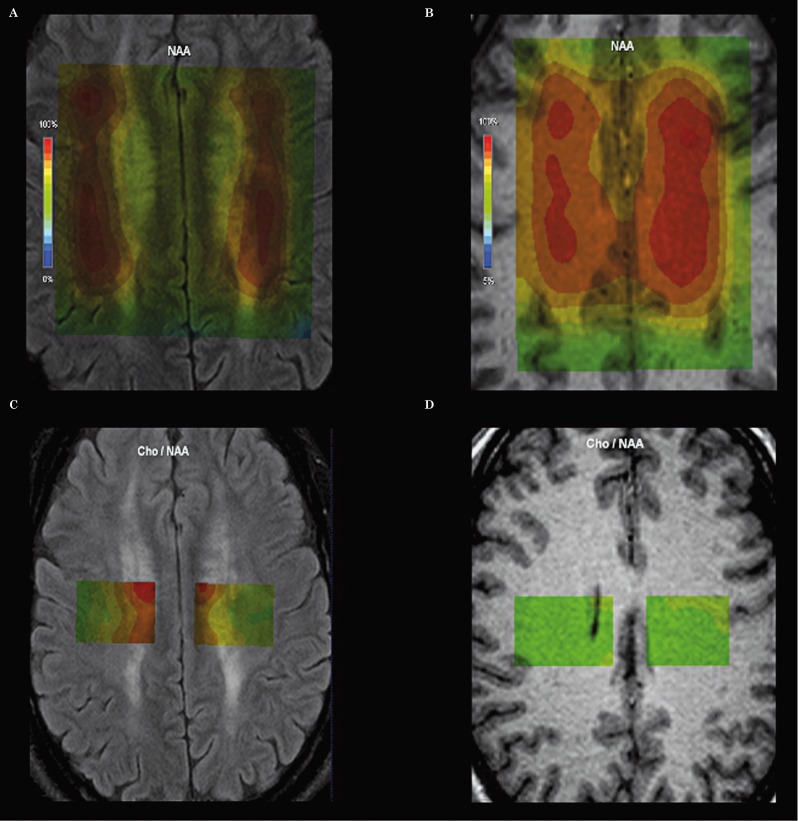
Leukoencephalopathy is a hallmark of mitochondrial neurogastrointestinal encephalomyopathy (MNGIE) a devastating disorder characterized by ptosis, ophthalmoparesis, gastrointestinal dysfunction and polyneuropathy. To characterize MNGIE-associated leukoencephalopathy and to correlate it with clinical, biochemical and molecular data, four MNGIE patients with heterogeneous clinical phenotypes (enteropathic arthritis, exercise intolerance, CIDP-like phenotype and typical presentation) were studied by magnetic resonance imaging (MRI) and magnetic resonance spectroscopy (MRS). Diffusion weighted imaging (DWI) with apparent diffusion coefficient (ADC) maps were also obtained. In two patients we also investigated the role of brain MRI in monitoring the evolution of leukoencephalopathy by performing follow-up imaging studies at an interval of one and two years. The extension and distribution of leukoencephalopathy were not clearly linked with age, phenotype or disease severity, and did not seem to be related to TYMP mutations, enzyme activity or pyrimidine levels. In the studied patients MRS revealed reduced N-acetyl-aspartate and increased choline signals. Although DWI appeared normal in all patients but one, ADC maps always showed moderate increased diffusivity. Leukoencephalopathy worsened over a two-year period in two patients, regardless of the clinical course, indicating a lack of correlation between clinical phenotype, size and progression of white matter abnormalities during this period. Brain MRI should be considered a very useful tool to diagnose both classical and atypical MNGIE. Serial MRIs in untreated and treated MNGIE patients will help to establish whether the leukoencephalopathy is a reversible condition or not.
Keywords: DWI; MNGIE; MRI; MRS; mitochondrial neurogastrointestinal encephalomyopathy; posterior reversible encephalopathy syndrome.
Figures
Similar articles
-
Evidence of enteric angiopathy and neuromuscular hypoxia in patients with mitochondrial neurogastrointestinal encephalomyopathy.Am J Physiol Gastrointest Liver Physiol. 2021 May 1;320(5):G768-G779. doi: 10.1152/ajpgi.00047.2021. Epub 2021 Mar 3. Am J Physiol Gastrointest Liver Physiol. 2021. PMID: 33655764 Free PMC article.
-
Mitochondrial neurogastrointestinal encephalomyopathy (MNGIE): case report with a new mutation.Eur J Pediatr. 2010 Nov;169(11):1375-8. doi: 10.1007/s00431-010-1237-0. Epub 2010 Jun 29. Eur J Pediatr. 2010. PMID: 20585803
-
Pitfalls in diagnosing mitochondrial neurogastrointestinal encephalomyopathy.J Inherit Metab Dis. 2011 Dec;34(6):1199-203. doi: 10.1007/s10545-011-9332-6. Epub 2011 Apr 19. J Inherit Metab Dis. 2011. PMID: 21503690
-
Novel Mutations of the TYMP Gene in Mitochondrial Neurogastrointestinal Encephalomyopathy: Case Series and Literature Review.J Mol Neurosci. 2021 Dec;71(12):2526-2533. doi: 10.1007/s12031-021-01822-w. Epub 2021 Apr 6. J Mol Neurosci. 2021. PMID: 33825174 Review.
-
Rare digestive disease: Mitochondrial neurogastrointestinal encephalomyopathy, review of the literature.J Dig Dis. 2024 Sep-Oct;25(9-10):624-631. doi: 10.1111/1751-2980.13317. Epub 2024 Dec 18. J Dig Dis. 2024. PMID: 39694028 Review.
Cited by
-
Overview of neuroimaging in primary mitochondrial disorders.Pediatr Radiol. 2025 Apr;55(4):765-791. doi: 10.1007/s00247-025-06172-y. Epub 2025 Feb 12. Pediatr Radiol. 2025. PMID: 39937244 Review.
-
Mitochondrial Neurogastrointestinal Encephalomyopathy (MNGIE-MTDPS1).J Clin Med. 2018 Oct 26;7(11):389. doi: 10.3390/jcm7110389. J Clin Med. 2018. PMID: 30373120 Free PMC article. Review.
-
Genes and Pathways Involved in Adult Onset Disorders Featuring Muscle Mitochondrial DNA Instability.Int J Mol Sci. 2015 Aug 5;16(8):18054-76. doi: 10.3390/ijms160818054. Int J Mol Sci. 2015. PMID: 26251896 Free PMC article. Review.
-
Safety and Efficacy of Erythrocyte Encapsulated Thymidine Phosphorylase in Mitochondrial Neurogastrointestinal Encephalomyopathy.J Clin Med. 2019 Apr 5;8(4):457. doi: 10.3390/jcm8040457. J Clin Med. 2019. PMID: 30959750 Free PMC article.
-
Mitochondrial neurogastrointestinal encephalomyopathy (MNGIE): Position paper on diagnosis, prognosis, and treatment by the MNGIE International Network.J Inherit Metab Dis. 2021 Mar;44(2):376-387. doi: 10.1002/jimd.12300. Epub 2020 Sep 8. J Inherit Metab Dis. 2021. PMID: 32898308 Free PMC article. Review.
References
-
- Nishino I, Spinazzola A, Hirano M. Thymidine phosphorylase gene mutations in MNGIE, a human mitochondrial disorder. Science. 1999;283:689–692. - PubMed
-
- Lara MC, Valentino ML, Torres-Torronteras J, et al. Mitochondrial neurogastrointestinal encephalomyopathy (MNGIE): biochemical features and therapeutic approaches. Biosci Rep. 2007;27:151–163. - PubMed
-
- Martí R, Verschuuren JJ, Buchman A, et al. Late-onset MNGIE due to partial loss of thymidine phosphorylase activity. Ann Neurol. 2005;58:649–652. - PubMed
-
- Hirano M, Silvestri G, Blake DM, et al. Mitochondrial neurogastrointestinal encephalomyopathy (MNGIE): clinical, biochemical, and genetic features of an autosomal recessive mitochondrial disorder. Neurology. 1994;44:721–727. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
