

Initial use of one or two antibiotics for critically ill patients with community-acquired pneumonia: impact on survival and bacterial resistance
- PMID: 24200097
- PMCID: PMC4056004
- DOI: 10.1186/cc13095
Initial use of one or two antibiotics for critically ill patients with community-acquired pneumonia: impact on survival and bacterial resistance
Abstract
Introduction: Several guidelines recommend initial empirical treatment with two antibiotics instead of one to decrease mortality in community-acquired pneumonia (CAP) requiring intensive-care-unit (ICU) admission. We compared the impact on 60-day mortality of using one or two antibiotics. We also compared the rates of nosocomial pneumonia and multidrug-resistant bacteria.
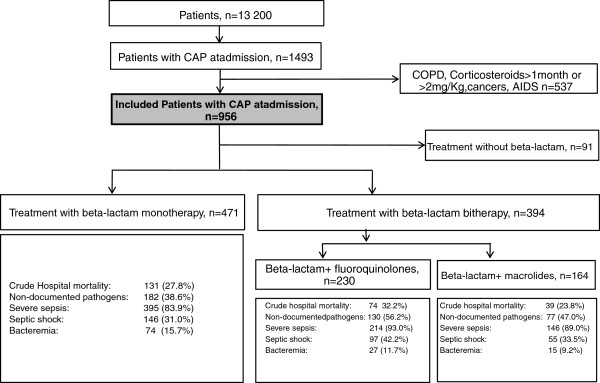
Methods: This is an observational cohort study of 956 immunocompetent patients with CAP admitted to ICUs in France and entered into a prospective database between 1997 and 2010.
Results: Initial adequate antibiotic therapy was significantly associated with better survival (subdistribution hazard ratio (sHR), 0.63; 95% confidence interval (95% CI), 0.42 to 0.94; P = 0.02); this effect was strongest in patients with Streptococcus pneumonia CAP (sHR, 0.05; 95% CI, 0.005 to 0.46; p = 0.001) or septic shock (sHR: 0.62; 95% CI 0.38 to 1.00; p = 0.05). Dual therapy was associated with a higher frequency of initial adequate antibiotic therapy. However, no difference in 60-day mortality was found between monotherapy (β-lactam) and either of the two dual-therapy groups (β-lactam plus macrolide or fluoroquinolone). The rates of nosocomial pneumonia and multidrug-resistant bacteria were not significantly different across these three groups.
Conclusions: Initial adequate antibiotic therapy markedly decreased 60-day mortality. Dual therapy improved the likelihood of initial adequate therapy but did not predict decreased 60-day mortality. Dual therapy did not increase the risk of nosocomial pneumonia or multidrug-resistant bacteria.
Figures
References
-
- Adrie C, Alberti C, Chaix-Couturier C, Azoulay E, De Lassence A, Cohen Y, Meshaka P, Cheval C, Thuong M, Troché G, Garrouste-Orgeas M, Timsit JF. Epidemiology and economic evaluation of severe sepsis in France: age, severity, infection site, and place of acquisition (community, hospital, or intensive care unit) as determinants of workload and cost. J Crit Care. 2005;17:46–58. doi: 10.1016/j.jcrc.2004.10.005. - DOI - PubMed
-
- Kumar A, Ellis P, Arabi Y, Roberts D, Light B, Parrillo JE, Dodek P, Wood G, Kumar A, Simon D, Peters C, Ahsan M, Chateau D. Cooperative Antimicrobial Therapy of Septic Shock Database Research Group. Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Chest. 2009;17:1237–1248. doi: 10.1378/chest.09-0087. - DOI - PubMed
-
- Rodríguez A, Mendia A, Sirvent JM, Barcenilla F, de la Torre-Prados MV, Solé-Violán J, Rello J. CAPUCI Study Group. Combination antibiotic therapy improves survival in patients with community-acquired pneumonia and shock. Crit Care Med. 2007;17:1493–1498. doi: 10.1097/01.CCM.0000266755.75844.05. - DOI - PubMed
-
- Lim WS, Baudouin SV, George RC, Hill AT, Jamieson C, Le Jeune I, Macfarlane JT, Read RC, Roberts HJ, Levy ML, Wani M, Woodhead MA. Pneumonia Guidelines Committee of the BTS Standards of Care Committee. BTS guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax. 2009;17:iii1–iii55. - PubMed
-
- Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, Dowell SF, File TM Jr, Musher DM, Niederman MS, Torres A, Whitney CG. Infectious Diseases Society of America; American Thoracic Society. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;17:S27–S72. doi: 10.1086/511159. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
