

Two decades of mortality trends among patients with severe sepsis: a comparative meta-analysis*
- PMID: 24201173
- PMCID: PMC4313930
- DOI: 10.1097/CCM.0000000000000026
Two decades of mortality trends among patients with severe sepsis: a comparative meta-analysis*
Abstract
Objectives: Trends in severe sepsis mortality derived from administrative data may be biased by changing International Classification of Diseases, 9th Revision, Clinical Modification, coding practices. We sought to determine temporal trends in severe sepsis mortality using clinical trial data that does not rely on International Classification of Diseases, 9th Revision, Clinical Modifications coding and compare mortality trends in trial data with those observed from administrative data.
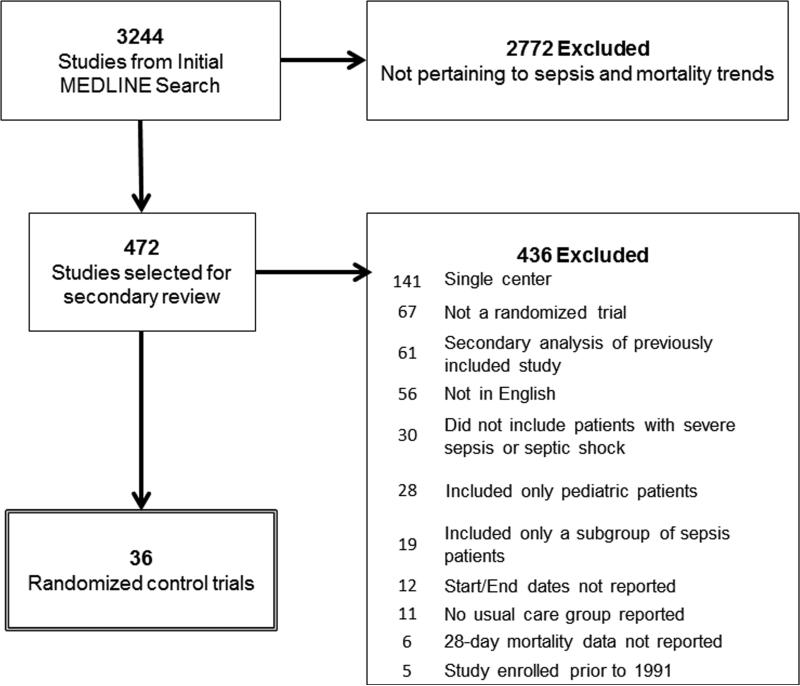
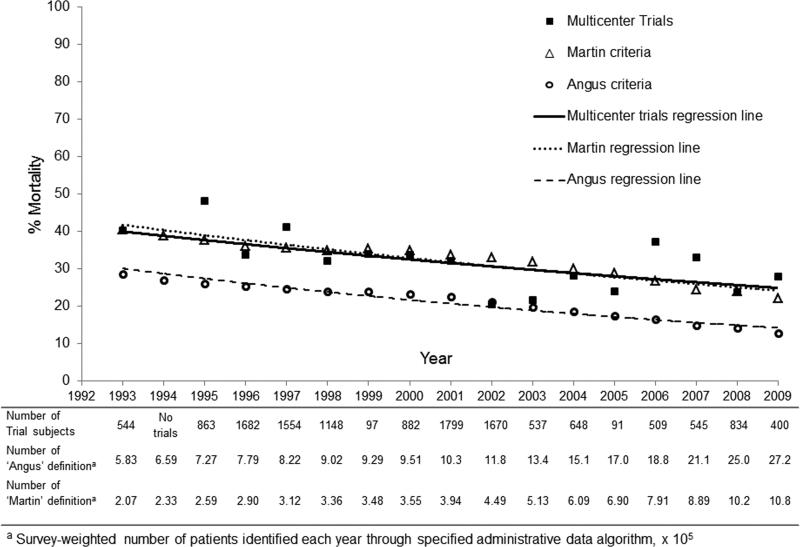
Design: We searched MEDLINE for multicenter randomized trials that enrolled patients with severe sepsis from 1991 to 2009. We calculated standardized mortality ratios for each trial from observed 28-day mortality of usual care participants and predicted mortality from severity-of-illness scores. To compare mortality trends from clinical trials to administrative data, we identified adult severe sepsis hospitalizations in the Nationwide Inpatient Sample, 1993-2009, using two previously validated algorithms.
Setting: In-patient.
Patients: Patients with severe sepsis or septic shock.
Interventions: None.
Measurements and main results: Of 3,244 potentially eligible articles, we included 36 multicenter severe sepsis trials, with a total of 14,418 participants in a usual care arm. Participants with severe sepsis receiving usual care had a 28-day mortality of 33.2%. Observed mortality decreased 3.0% annually (95% CI, 0.8%-5.0%; p = 0.009), decreasing from 46.9% (standardized mortality ratio 0.94; 95% CI, 0.86-1.03) during years 1991-1995 to 29% (standardized mortality ratio 0.53; 95% CI, 0.50-0.57) during years 2006-2009 (3.0% annual change). Trends in hospital mortality among patients with severe sepsis identified from administrative data (Angus definition, 4.7% annual change; 95% CI, 4.1%-5.3%; p = 0.69 and Martin definition, 3.5% annual change; 95% CI, 3.0%-4.1%; p = 0.97) were similar to trends identified from clinical trials.
Conclusion: Since 1991, patients with severe sepsis enrolled in usual care arms of multicenter randomized trials have experienced decreasing mortality. The mortality trends identified in clinical trial participants appear similar to those identified using administrative data and support the use of administrative data to monitor mortality trends in patients with severe sepsis.
Figures
Comment in
-
Can administrative data be used to consistently measure the burden of sepsis?*.Crit Care Med. 2014 Mar;42(3):747-9. doi: 10.1097/CCM.0000000000000075. Crit Care Med. 2014. PMID: 24534970 No abstract available.
References
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–1554. - PubMed
-
- Dombrovskiy VY, Martin AA, Sunderram J, Paz HL. Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: A trend analysis from 1993 to 2003. Crit Care Med. 2007;35:1244–1250. - PubMed
-
- Kumar G, Kumar N, Taneja A, et al. Nationwide trends of severe sepsis in the 21st Century (2000-2007). Chest. 2011;140:1223–1231. - PubMed
-
- Lagu T, Rothberg MB, Shieh MS, Pekow PS, Steingrub JS, Lindenauer PK. Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Crit Care Med. 2011;40:754–61. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
